Aetna Medicare Provider Appeal Form
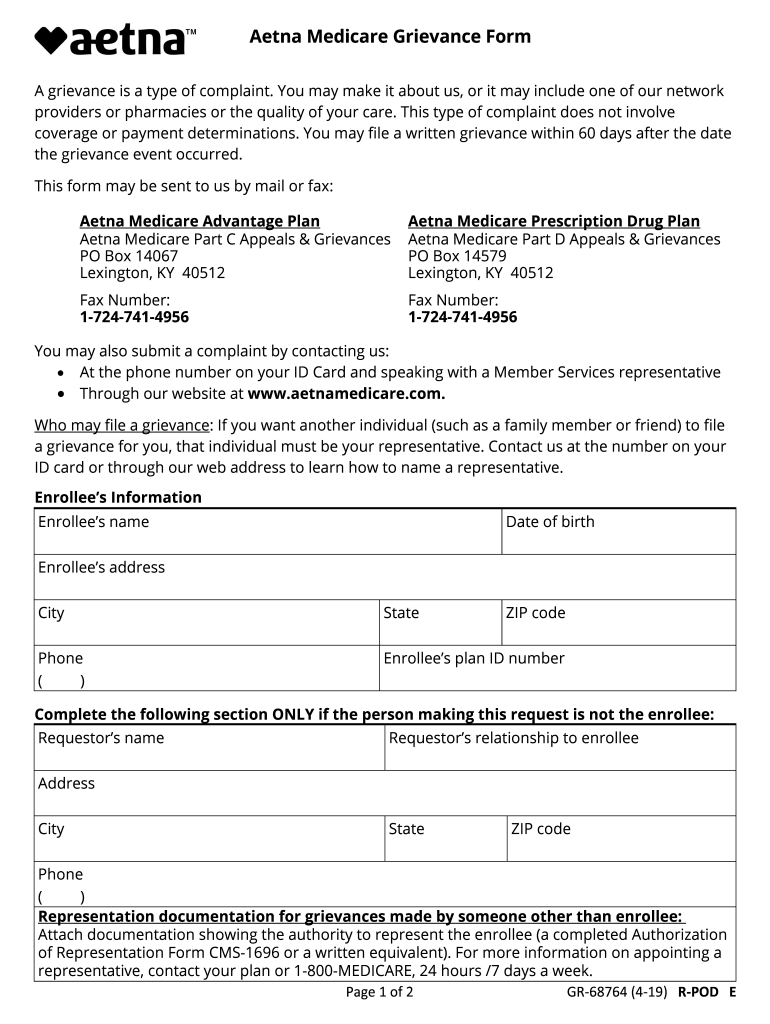
Aetna Medicare Provider Appeal Form - File a complaint about the quality of care or other services you get from us or from a medicare provider. You have 60 calendar days from the date of your denial to ask us for an appeal. Get a medicare advantage provider complaint and appeal form (pdf) get a non medicare advantage provider complaint and appeal form (pdf) to facilitate handling: Address, phone number and practice changes. Make sure to include any information that will support your appeal. 711) hospital discharge appeal notices (cms website) log in use our secure provider website to access electronic transactions and valuable resources to support your organization. Coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals. There are different steps to take based on the type of request you have. Aetna medicare appeals po box 14067 lexington, ky 40512. Web complaint and appeal request note:
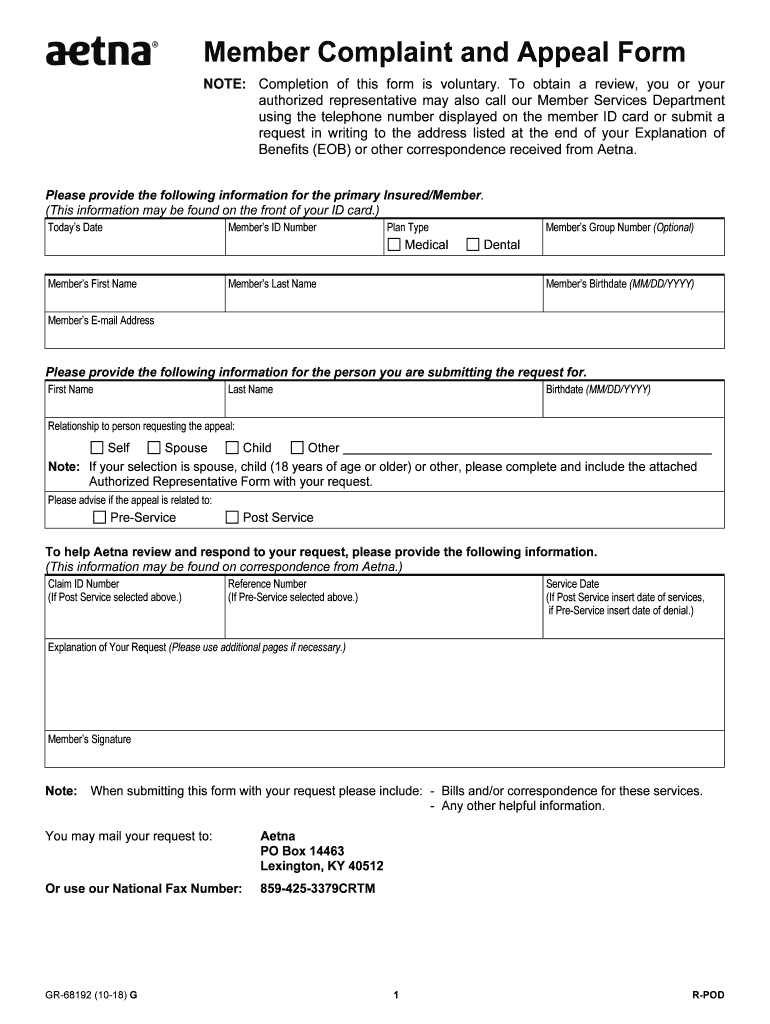
To obtain a review, you’ll need to submit this form. Appeals must be submitted by mail/fax, using the provider complaint and appeal form. Web find forms and applications for health care professionals and patients, all in one place. Find a form find forms for claims, payment, billing, medicare, pharmacy and more. Web complaint and appeal request note: Make sure to include any information that will support your appeal. Make sure to include any information that will support your appeal. Requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. To obtain a review, you’ll need to submit this form. Get a medicare advantage provider complaint and appeal form (pdf) get a non medicare advantage provider complaint and appeal form (pdf) to facilitate handling:
Web complaint and appeal request note: Appeals must be submitted by mail/fax, using the provider complaint and appeal form. You must complete this form. Web you may mail your request to: Claim id number (s) reference number/authorization number. Get a medicare advantage provider complaint and appeal form (pdf) get a non medicare advantage provider complaint and appeal form (pdf) to facilitate handling: Aetna medicare appeals po box 14067 lexington, ky 40512. 711) hospital discharge appeal notices (cms website) log in use our secure provider website to access electronic transactions and valuable resources to support your organization. Make sure to include any information that will support your appeal. You have 60 calendar days from the date of your denial to ask us for an appeal.
Aetna Medicare Complaint Team Fill Out and Sign Printable PDF
Find a form find forms for claims, payment, billing, medicare, pharmacy and more. Appeals must be submitted by mail/fax, using the provider complaint and appeal form. This form may be sent to us by mail or fax: Web (this information may be found on correspondence from aetna.) you may use this form to appeal multiple dates of service for the.
20182021 Form Aetna GR68192 Fill Online, Printable, Fillable, Blank
Appeals must be submitted by mail/fax, using the provider complaint and appeal form. Aetna medicare appeals po box 14067 lexington, ky 40512. Address, phone number and practice changes. This form may be sent to us by mail or fax: Find a form find forms for claims, payment, billing, medicare, pharmacy and more.
FREE 10+ Sample Medicare Forms in PDF MS Word
You may also ask us for an appeal through our website at www.aetnamedicare.com. Aetna medicare appeals po box 14067 lexington, ky 40512. You must complete this form. There are different steps to take based on the type of request you have. File a complaint about the quality of care or other services you get from us or from a medicare.
Medicare Medical Claim Reimbursement Form Aetna Form Resume
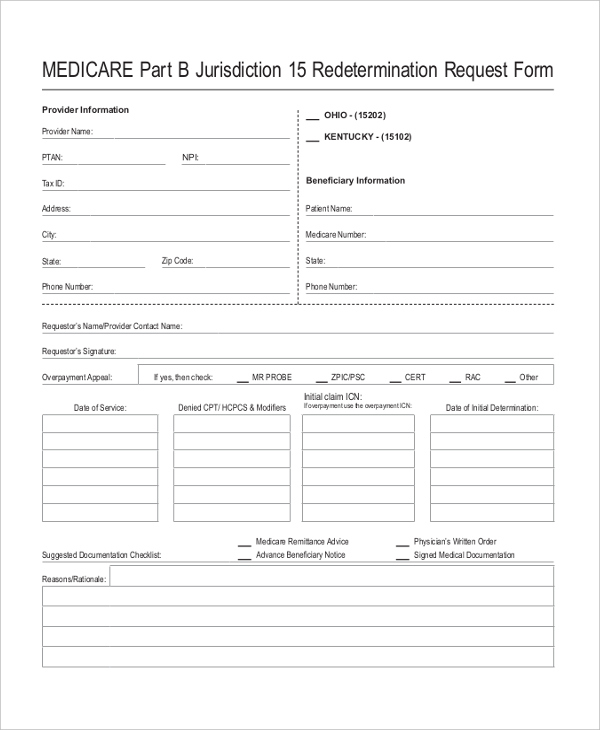
You must complete this form. Requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Make sure to include any information that will support your appeal. Aetna medicare appeals po box 14067 lexington, ky 40512. Web reconsiderations can be submitted online, by phone or by mail/fax.

Aetna Appeal Letter Sample Templates
Coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals. You must complete this form. You have 60 calendar days from the date of your denial to ask us for an appeal. To obtain a review, you’ll need to submit this form. Or use our national fax number:

Aetna Appeal Letter Sample Templates
Requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Web reconsiderations can be submitted online, by phone or by mail/fax. File a complaint about the quality of care or other services you get from us or from a medicare provider. Web complaint and appeal request note: Make sure to include any information that will support your.

Information Regarding Aetna Medicare Advantage 2021
You must complete this form. An appeal is a formal way of asking us to review and change a coverage decision we made. Aetna medicare appeals po box 14067 lexington, ky 40512. Coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals. Web complaint and appeal request note:
Aetna Reconsideration Form Fill Online, Printable, Fillable, Blank
This form may be sent to us by mail or fax: Make sure to include any information that will support your appeal. Web find forms and applications for health care professionals and patients, all in one place. 711) hospital discharge appeal notices (cms website) log in use our secure provider website to access electronic transactions and valuable resources to support.

Aetna GR67902 2004 Fill and Sign Printable Template Online US
To obtain a review, you’ll need to submit this form. Address, phone number and practice changes. Web complaint and appeal request note: There are different steps to take based on the type of request you have. You may mail your request to:
Index of Network Provider
You must complete this form. Web find forms and applications for health care professionals and patients, all in one place. File a complaint about the quality of care or other services you get from us or from a medicare provider. You must complete this form. There are different steps to take based on the type of request you have.
Aetna Medicare Appeals Po Box 14067 Lexington, Ky 40512.
Or use our national fax number: Make sure to include any information that will support your appeal. Appeals must be submitted by mail/fax, using the provider complaint and appeal form. Find a form find forms for claims, payment, billing, medicare, pharmacy and more.
You May Mail Your Request To:
File a complaint about the quality of care or other services you get from us or from a medicare provider. 711) hospital discharge appeal notices (cms website) log in use our secure provider website to access electronic transactions and valuable resources to support your organization. You must complete this form. Claim id number (s) reference number/authorization number.
You Have 60 Calendar Days From The Date Of Your Denial To Ask Us For An Appeal.
Make sure to include any information that will support your appeal. To obtain a review, you’ll need to submit this form. Web reconsiderations can be submitted online, by phone or by mail/fax. Web find forms and applications for health care professionals and patients, all in one place.
There Are Different Steps To Take Based On The Type Of Request You Have.
Web complaint and appeal request note: Web (this information may be found on correspondence from aetna.) you may use this form to appeal multiple dates of service for the same member. An appeal is a formal way of asking us to review and change a coverage decision we made. Coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals.