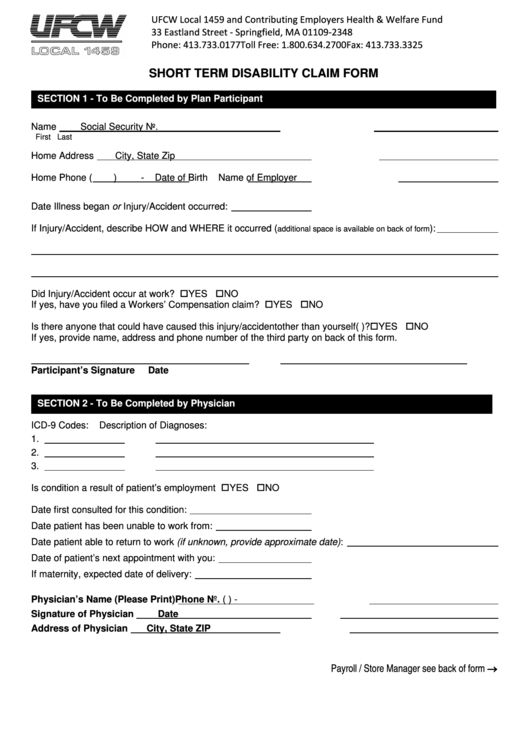
Aflac Short Term Disability Claim Form
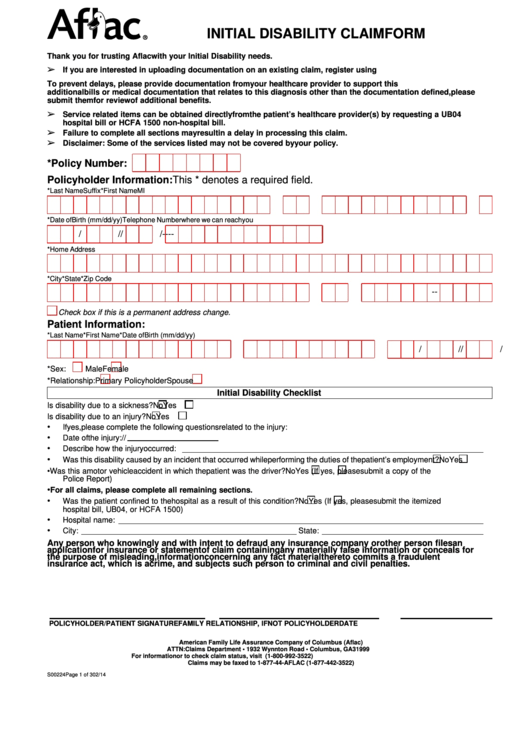
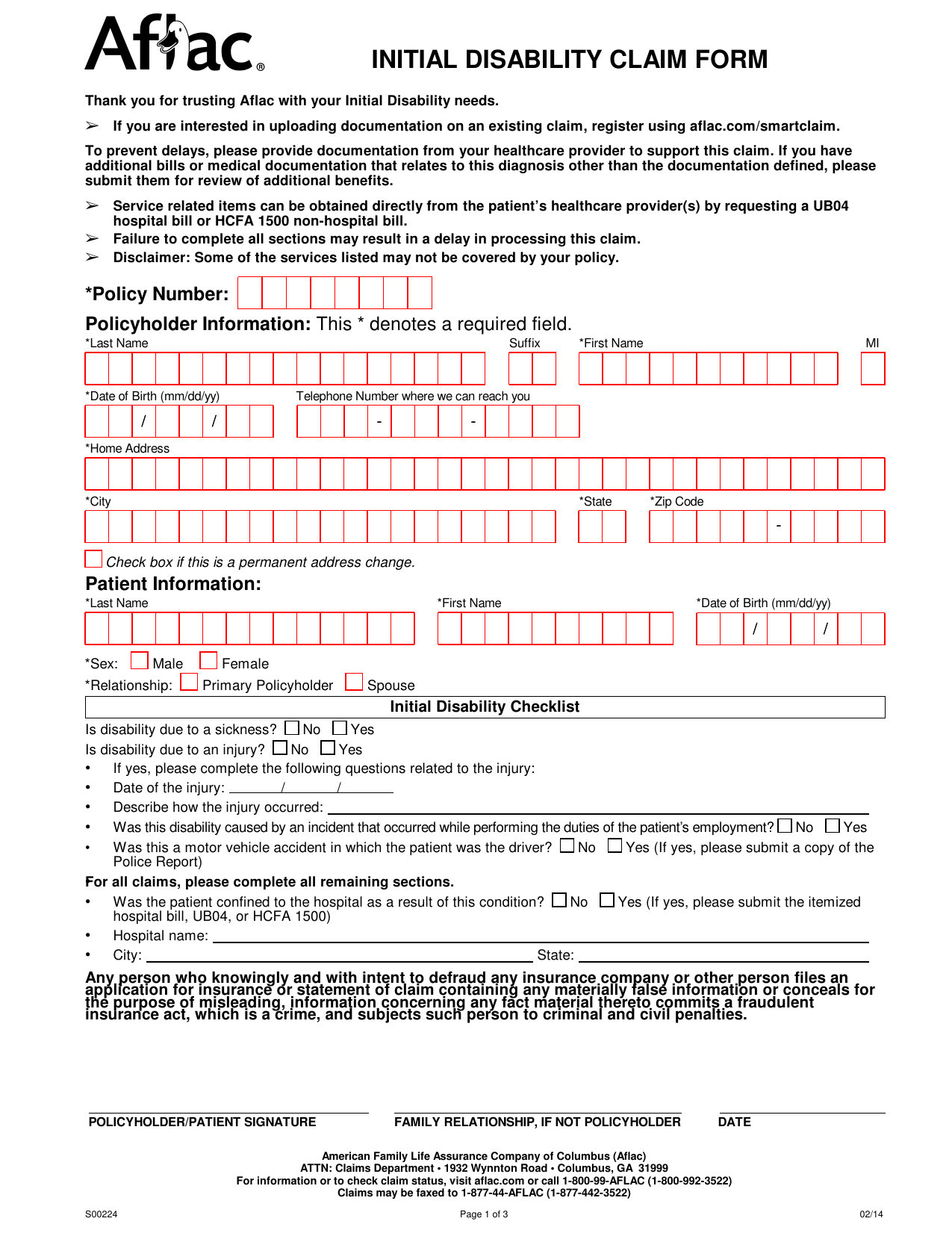
Aflac Short Term Disability Claim Form - Web for assistance or information, call 1.800.99.aflac (1.800.992.3522). Nt (forms are to be completed on or after disability date to avoid processing delays) policy holder’s name: Web for claim forms, visit our web site at aflac.com. *last name suffix *first name *date of birth (mm/dd/yy) / / patient information: It is not a substitute for hospital or medical expense insurance, a health mainten ance organization (hmo) contract, or major medical expense insurance. Web download aflac short term disability claim form, also known as aflac initial disability claim form. Web short term disability claim form. Short term disability/long term disability claim form *last name *first name *date of birth (mm/dd/yy) / / physician information: Please sign and return the attached hipaa.
This is a supplement to health insurance. Short term disability/long term disability claim form This * denotes a required field. Consider filing online for faster claims payment! Web aflac group disability claim form_2020 post office box 84075 * columbus, ga. Web short term disability claim form. It is not a substitute for hospital or medical expense insurance, a health mainten ance organization (hmo) contract, or major medical expense insurance. • it’s sold on an individual basis. If you are eligible for medicare, review the “guide to health insurance for people with medicare” available from aflac. Policyholder’s statement (forms are to be completed on or after disability date to avoid processing delays)
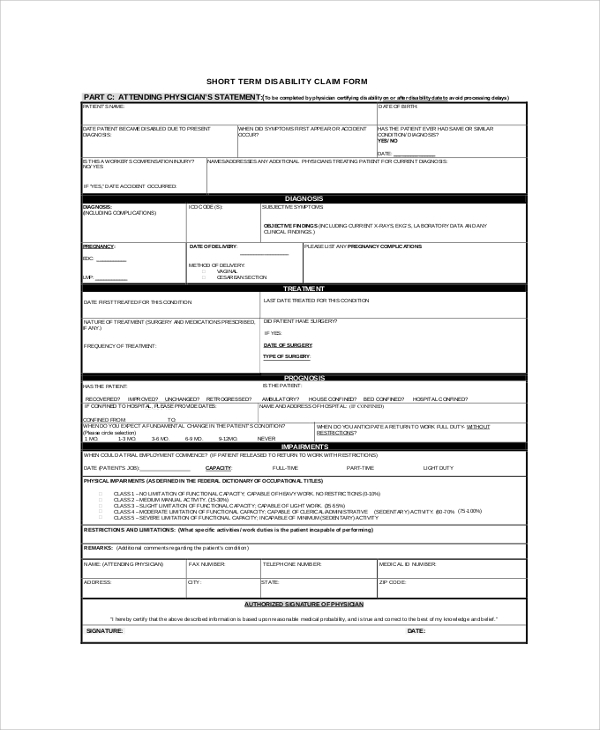
Web notice of claim for short term disability benefits long term disability benefits employee’s statement (to be completed by employee. Policyholder’s statement (forms are to be completed on or after disability date to avoid processing delays) *last name *first name *date of birth (mm/dd/yy) / / physician information: Web claims checklist claims checklist helpful tips: Web form a57601coh 1 of 9 a576c01coh.2. My coverage here you’ll find a copy of your policy and benefit details to see what’s covered and benefit amounts. Attending physician’s statement to be completed byphysician certifying disabilityon or after disability dateto. Web file your claim via fax or mail. Web short term disability claim form. Consider filing online for faster claims payment!
FREE 8+ Sample Aflac Claim Forms in PDF
Web form a57601coh 1 of 9 a576c01coh.2. Include tax records, at the time of claim. This * denotes a required field. If uploading a picture from your phone, please only submit the medical documentation for your proof of services. That means no medical questionnaire is required.

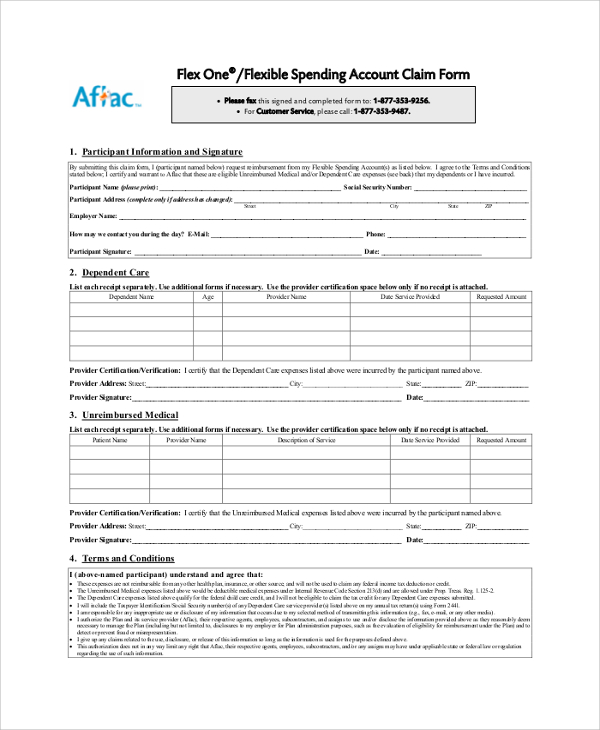
Fill Free fillable Aflac Insurance PDF forms
To be completed by aflac associate/agent. Please sign and return the attached hipaa. This * denotes a required field. For claim forms, visit our web site at aflac.com. If uploading a picture from your phone, please only submit the medical documentation for your proof of services.
FREE 8+ Sample Aflac Claim Forms in PDF
Web notice of claim for short term disability benefits long term disability benefits employee’s statement (to be completed by employee. To be completed by aflac associate/agent. Annual income must be $9,000 or greater for coverage to be issued. Web form a57601coh 1 of 9 a576c01coh.2. *last name suffix *first name *date of birth (mm/dd/yy) / / patient information:
Cincinnati Ins Co Claims Aflac Injury Claim
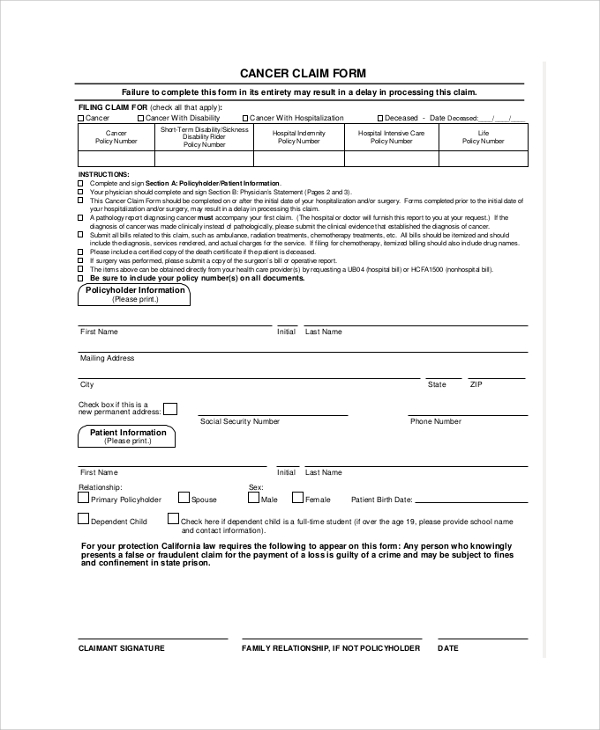
This form is used to file a claim for short term disability. Web claims checklist claims checklist helpful tips: *last name *first name *date of birth (mm/dd/yy) / / physician information: Policyholder’s statement (forms are to be completed on or after disability date to avoid processing delays) Web download aflac short term disability claim form, also known as aflac initial.

Fill Free fillable Aflac Insurance PDF forms
Web for assistance or information, call 1.800.99.aflac (1.800.992.3522). My coverage here you’ll find a copy of your policy and benefit details to see what’s covered and benefit amounts. *last name *first name *date of birth (mm/dd/yy) / / physician information: If uploading a picture from your phone, please only submit the medical documentation for your proof of services. Web for.
Download Aflac Short Term Disability Claim Form/ Initial Disability
Web for assistance or information, call 1.800.99.aflac (1.800.992.3522). If you are eligible for medicare, review the “guide to health insurance for people with medicare” available from aflac. When taking photo copies of the documents make sure the document is flat. Include tax records, at the time of claim. That means no medical questionnaire is required.
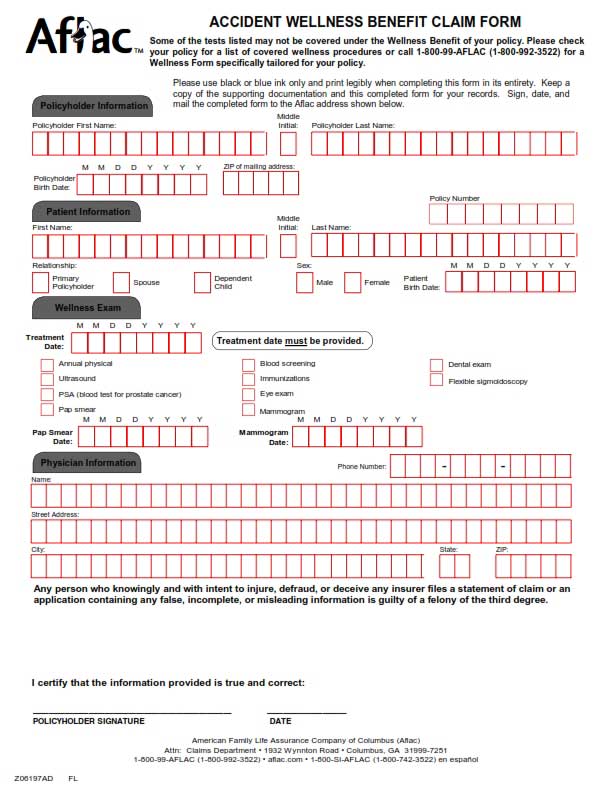
Aflac Wellness Claim Form Printable
*last name *first name *date of birth (mm/dd/yy) / / physician information: Web download aflac short term disability claim form, also known as aflac initial disability claim form. For claim forms, visit our web site at aflac.com. Web aflac group disability claim form_2020 post office box 84075 * columbus, ga. Web file your claim via fax or mail.
Aflac Claim Forms Printable Master of Documents
This * denotes a required field. Consider filing online for faster claims payment! Web short term disability claim form. *last name *first name *date of birth (mm/dd/yy) / / physician information: If uploading a picture from your phone, please only submit the medical documentation for your proof of services.
How Do Insurance Companies Pay Out Claims Aflac Accident Claim Form
Web claims checklist claims checklist helpful tips: You choose the plan that’s right for you based on your financial needs and income. For claim forms, visit our web site at aflac.com. Policyholder’s statement (forms are to be completed on or after disability date to avoid processing delays) Nt (forms are to be completed on or after disability date to avoid.
Is Aflac Short Term Disability Taxable Gianna Jordan's Blog
Web form a57601coh 1 of 9 a576c01coh.2. Web for claim forms, visit our web site at aflac.com. If disability, is later, determined to be for a longer term, there will be follow up forms required at that time. Flatten documents that have been folded or crumbled before uploading. Attending physician’s statement to be completed byphysician certifying disabilityon or after disability.
If You Are Eligible For Medicare, Review The “Guide To Health Insurance For People With Medicare” Available From Aflac.
This * denotes a required field. Nt (forms are to be completed on or after disability date to avoid processing delays) policy holder’s name: If disability, is later, determined to be for a longer term, there will be follow up forms required at that time. My claims follow your claim from start to finish and receive alerts if we need additional information through our integrated claim status tracker.
Flatten Documents That Have Been Folded Or Crumbled Before Uploading.
Web short term disability claim form. To avoid delay, all questions must be answered.) please complete both pages of this form for pregnancy disability only: When taking photo copies of the documents make sure the document is flat. If uploading a picture from your phone, please only submit the medical documentation for your proof of services.
Short Term Disability/Long Term Disability Claim Form
This form is used to file a claim for short term disability. Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the attached authorization. *last name suffix *first name *date of birth (mm/dd/yy) / / patient information: You choose the plan that’s right for you based on your financial needs and income.
This * Denotes A Required Field.
Web file your claim via fax or mail. My coverage here you’ll find a copy of your policy and benefit details to see what’s covered and benefit amounts. That means no medical questionnaire is required. Web download aflac short term disability claim form, also known as aflac initial disability claim form.