Colonial Life Universal Claim Form
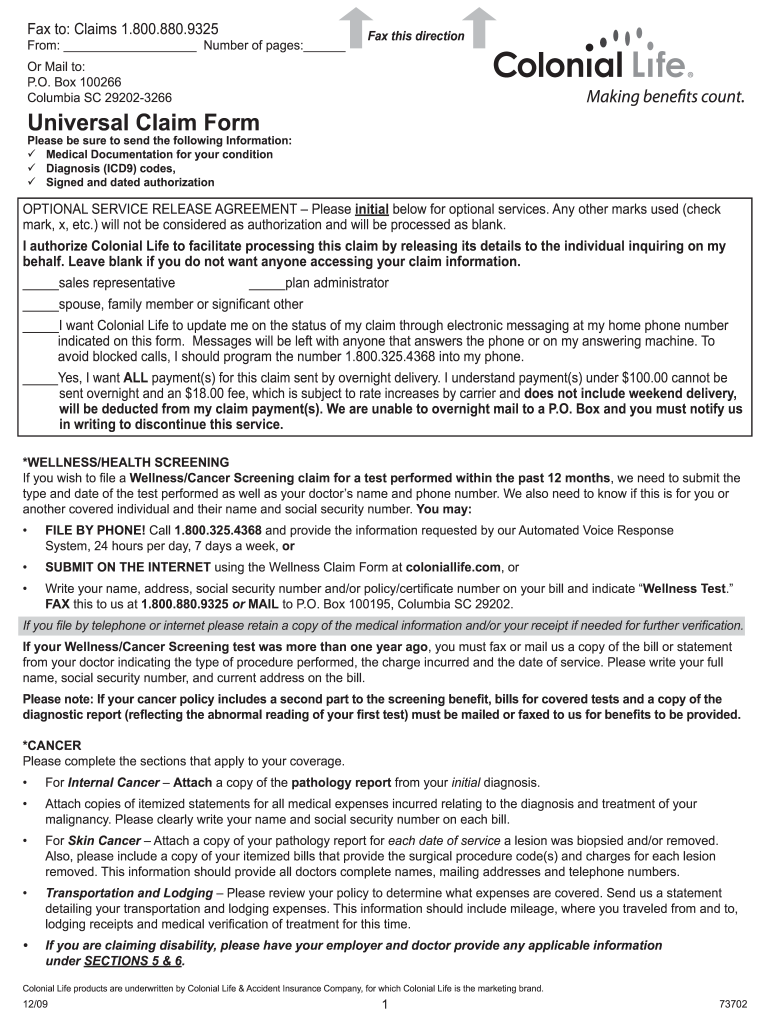
Colonial Life Universal Claim Form - The policies or their provisions may vary or be unavailable in some states. Claimant’s name, date of birth, ssn (if other than primary insured) date of diagnosis. Web your name, date of birth, social security number (ssn) and address. Primary doctor information and treating doctor (if different) diagnosis from your doctor. Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Web file colonial life insurance paper claim forms | colonial life. Web colonial life & accident insurance companyuniversal claim form fax: Web colonial life & accident insurance company, columbia, sc | universal claim form | fax: _____sales representative _____ plan administrator _____spouse, family member or significant other Use the cross or check marks in the top toolbar to select your answers in the list boxes.
Web the universal claim form. Box 100195, columbia, sc 29202 from: Use get form or simply click on the template preview to open it in the editor. Web your name, date of birth, social security number (ssn) and address. _____sales representative _____ plan administrator _____spouse, family member or significant other Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Bills or proof of treatment. Loss of life (death) notification form. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web file colonial life insurance paper claim forms | colonial life.
Web colonial life & accident insurance company, columbia, sc | universal claim form | fax: Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Web file colonial life insurance paper claim forms | colonial life. Use get form or simply click on the template preview to open it in the editor. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web i authorize colonial life to facilitate processing this claim by releasing its details to the individual inquiring on my behalf. Loss of life (death) notification form. Box 100195, columbia, sc 29202 from: Cancellation/surrender of your life policy. The policies or their provisions may vary or be unavailable in some states.

20192022 Colonial Life Form 67715 Fill Online, Printable, Fillable
Web the universal claim form. _____sales representative _____ plan administrator _____spouse, family member or significant other Use the cross or check marks in the top toolbar to select your answers in the list boxes. The form also provides helpful tips about the. Claimant’s name, date of birth, ssn (if other than primary insured) date of diagnosis.
FREE 32+ Claim Form Templates in PDF Excel MS Word
Claimant’s name, date of birth, ssn (if other than primary insured) date of diagnosis. Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Bills or proof of treatment. _____sales representative _____ plan administrator _____spouse, family.

File Colonial Life Insurance Claim Forms Colonial Life
Web colonial life & accident insurance company, columbia, sc | universal claim form | fax: The form also provides helpful tips about the. Primary doctor information and treating doctor (if different) diagnosis from your doctor. Loss of life (death) notification form. Use get form or simply click on the template preview to open it in the editor.
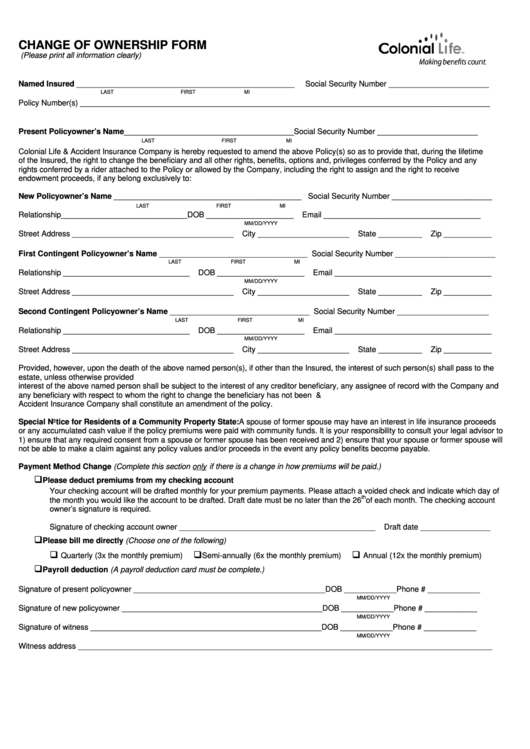
Form 1707516 Download Fillable PDF or Fill Online Change of
Web i authorize colonial life to facilitate processing this claim by releasing its details to the individual inquiring on my behalf. _____sales representative _____ plan administrator _____spouse, family member or significant other Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web your name, date of birth, social security number (ssn).
Fillable Colonial Life Health/wellness Screening Claim Form 2015
Leave blank if you do not want anyone accessing your claim information. Web the universal claim form. The policies or their provisions may vary or be unavailable in some states. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Primary doctor information and treating doctor (if different) diagnosis from your doctor.
Colonial Life Forms Fill Out and Sign Printable PDF Template signNow
Web your name, date of birth, social security number (ssn) and address. Web file colonial life insurance paper claim forms | colonial life. Loss of life (death) notification form. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Box 100195, columbia, sc 29202 from:
Colonial Life Disability Claim Form Fill Out and Sign Printable PDF
Web colonial life & accident insurance companyuniversal claim form fax: Web i authorize colonial life to facilitate processing this claim by releasing its details to the individual inquiring on my behalf. _____sales representative _____ plan administrator _____spouse, family member or significant other Web file colonial life insurance paper claim forms | colonial life. Primary doctor information and treating doctor (if.
Claim Form Universal Claim Form
_____sales representative _____ plan administrator _____spouse, family member or significant other Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Cancellation/surrender of your life policy. Web colonial life & accident insurance company, columbia, sc | universal claim form | fax: Box 100195, columbia, sc 29202 from:

Colonial Life Printable Claim Forms Printable Word Searches
Web colonial life & accident insurance companyuniversal claim form fax: Web the universal claim form. Start completing the fillable fields and carefully type in required information. Web your name, date of birth, social security number (ssn) and address. Use get form or simply click on the template preview to open it in the editor.
Top 21 Colonial Life Forms And Templates free to download in PDF format
Bills or proof of treatment. The form also provides helpful tips about the. The policies or their provisions may vary or be unavailable in some states. Web colonial life insurance products are underwritten by colonial life & accident insurance company, columbia, sc. Box 100195, columbia, sc 29202 from:
Cancellation/Surrender Of Your Life Policy.
Web the universal claim form. Box 100195, columbia, sc 29202 from: The form also provides helpful tips about the. Web colonial life & accident insurance company, columbia, sc | universal claim form | fax:
Primary Doctor Information And Treating Doctor (If Different) Diagnosis From Your Doctor.
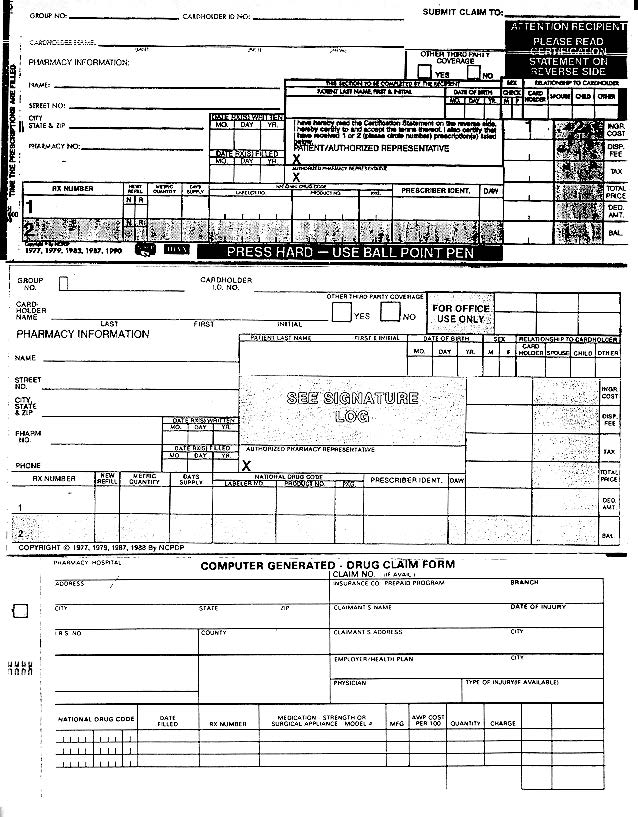
Web your name, date of birth, social security number (ssn) and address. Claimant’s name, date of birth, ssn (if other than primary insured) date of diagnosis. Box 100195, columbia, sc 29202 from: Bills or proof of treatment.
Web Colonial Life Insurance Products Are Underwritten By Colonial Life & Accident Insurance Company, Columbia, Sc.
Web file colonial life insurance paper claim forms | colonial life. Use get form or simply click on the template preview to open it in the editor. The policies have exclusions and limitations which may. Loss of life (death) notification form.
Start Completing The Fillable Fields And Carefully Type In Required Information.
Web i authorize colonial life to facilitate processing this claim by releasing its details to the individual inquiring on my behalf. Leave blank if you do not want anyone accessing your claim information. The policies or their provisions may vary or be unavailable in some states. _____sales representative _____ plan administrator _____spouse, family member or significant other