Express Scripts Appeal Form Non Medicare
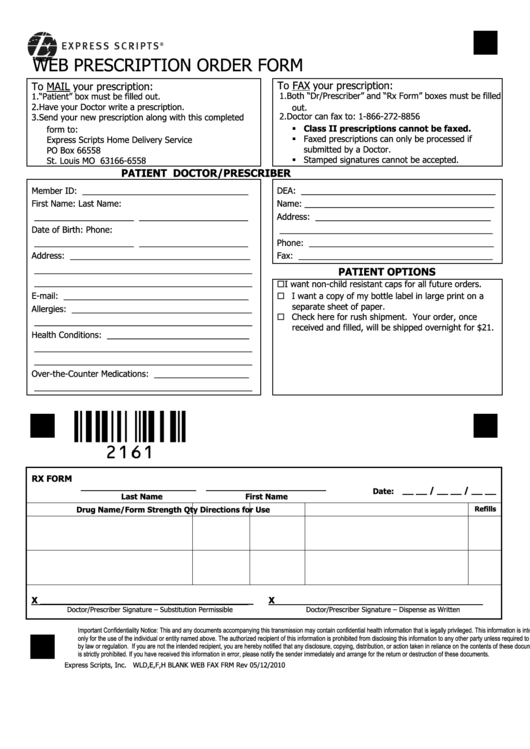
Express Scripts Appeal Form Non Medicare - Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; You recentlycontacted us to request coverage beyond your plan’s standard benefit. Web express scripts 1.877.328.9799 attn: Easier to use for prescribers, nurses and office. Depending on your plan, you may. Web members include those who have express scripts prescription benefits through their employer, health plan, or directly via medicare part d. Web express scripts offers epa options. Click here to get started. General express scripts request form (pdf) if you are a minnesota physician, please submit. Faster to send and get reviews.
We have received your pricing inquiry. Providers may use epa through. Be postmarked or received by. Web express scripts 1.877.328.9799 attn: Express scripts or rdt will respond in writing to you and/or your physician with a letter explaining the outcome of the appeal. General express scripts request form (pdf) if you are a minnesota physician, please submit. Web request an appeal what’s the form called? Web because we, express scripts, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Depending on your plan, you may. Use this contact information if you need to file an appeal if your coverage review is denied.
General express scripts request form (pdf) if you are a minnesota physician, please submit. Be in writing and signed, state specifically why you disagree, include a copy of the claim decision, and; Web express scripts offers epa options. Faster to send and get reviews. Web to initiate the coverage review process or an appeal of a previously declined coverage review request, please use the resources below: Read latest notifications, file pricing appeals and search express scripts claims and patient coverage for your pharmacy customers. Web your appeal must: Prescription drug coverage this application for second level appeal should be. Web express scripts resources for pharmacists. Express scripts or rdt will respond in writing to you and/or your physician with a letter explaining the outcome of the appeal.

Understanding Your Part D Explanation of Benefits Roadmap For Medicare
Depending on your plan, you may. You may ask for a review when you. Read latest notifications, file pricing appeals and search express scripts claims and patient coverage for your pharmacy customers. Web members include those who have express scripts prescription benefits through their employer, health plan, or directly via medicare part d. Faster to send and get reviews.
Top 16 Express Scripts Forms And Templates free to download in PDF format
Click here to get started. Read latest notifications, file pricing appeals and search express scripts claims and patient coverage for your pharmacy customers. Pharmacist resource center pricing inquiry received thank you for contacting express scripts pharmacy services. Web to initiate the coverage review process or an appeal of a previously declined coverage review request, please use the resources below: We.

57 HQ Images Express Scripts Appeal Form Express Scripts Prior
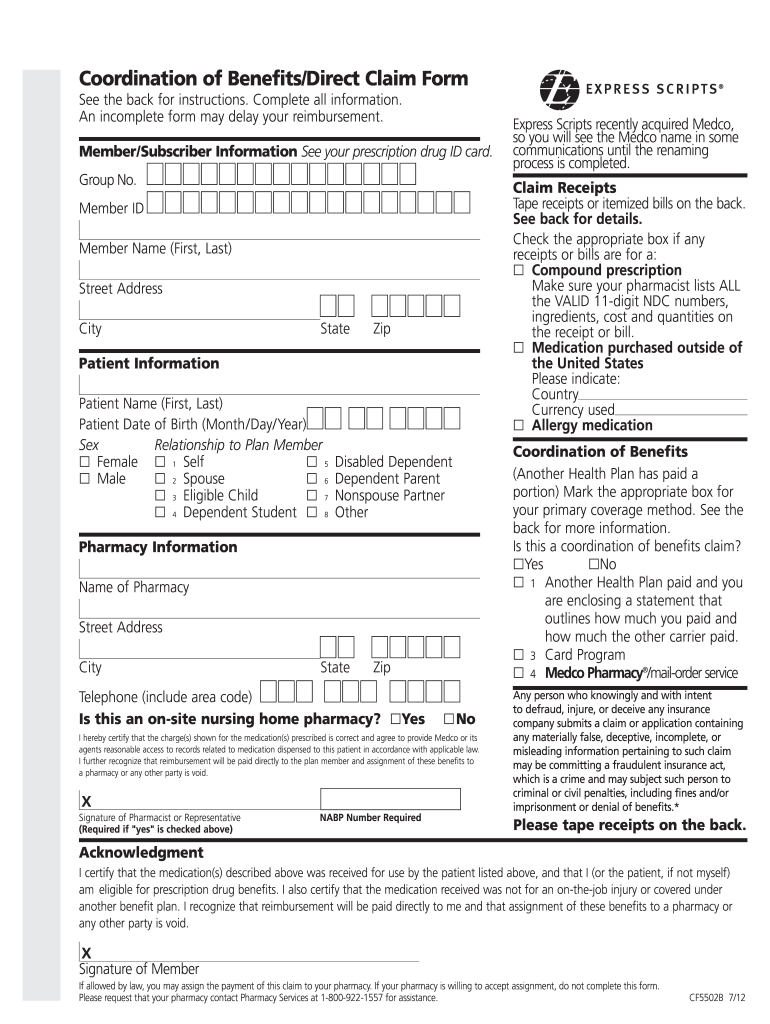
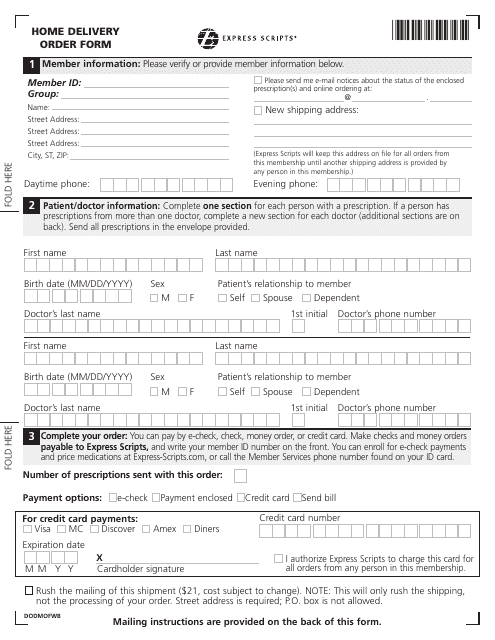
Requesting an appeal (redetermination) if you disagree with. Web members include those who have express scripts prescription benefits through their employer, health plan, or directly via medicare part d. Web express scripts manages your prescription drug benefit at the request of your health plan. Web mail your request with the above information to: Use this contact information if you need.

True Scripts Prior Authorization form New Express Scripts Prior
Web because we, express scripts, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Faster to send and get reviews. Requesting an appeal (redetermination) if you disagree with. Providers may use epa through. Web members include those who have express scripts prescription benefits through.

Express Scripts Prior Auth Form Unique Humana Prior
Web mail your request with the above information to: Web because we, express scripts, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Web express scripts offers epa options. Web express scripts 1.877.328.9799 attn: Faster to send and get reviews.
Express Scripts Appeal Form Fill Out and Sign Printable PDF Template
Web express scripts 1.877.328.9799 attn: Web express scripts resources for pharmacists. Be postmarked or received by. Web express scriptsapplication for second level appeal: Web epa is the preferred method to submit prior authorization requests to express scripts for pharmacy benefit drugs.
57 HQ Images Express Scripts Appeal Form Express Scripts Prior
Web an appeal, or redetermination, is a formal way to ask the plan to review a coverage decision about health care services and/or prescription drugs. Web members include those who have express scripts prescription benefits through their employer, health plan, or directly via medicare part d. Click here to get started. Easier to use for prescribers, nurses and office. Faster.
Vizio Class Action Lawsuit Claim Form Express Scripts Claims Address
Web express scriptsapplication for second level appeal: Web to initiate the coverage review process or an appeal of a previously declined coverage review request, please use the resources below: Prescription drug coverage this application for second level appeal should be. Web express scripts resources for pharmacists. Use this contact information if you need to file an appeal if your coverage.
Silver Scripts Prior Auth Form amulette
Web your appeal must: Web express scriptsapplication for second level appeal: Read latest notifications, file pricing appeals and search express scripts claims and patient coverage for your pharmacy customers. Depending on your plan, you may. Be postmarked or received by.
Express Scripts Fax Form Fill and Sign Printable Template Online US
Web express scripts offers epa options. Web initial coverage review purpose: Web express scripts resources for pharmacists. You may ask for a review when you. Web because we, express scripts, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our.
Be In Writing And Signed, State Specifically Why You Disagree, Include A Copy Of The Claim Decision, And;
Web now is a great time for you to make the switch to electronic prior authorization (epa). Express scripts or rdt will respond in writing to you and/or your physician with a letter explaining the outcome of the appeal. Web because we, express scripts, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Web express scripts manages your prescription drug benefit at the request of your health plan.
Web Express Scripts Resources For Pharmacists.
Be postmarked or received by. Web express scripts 1.877.328.9799 attn: Use this contact information if you need to file an appeal if your coverage review is denied. Easier to use for prescribers, nurses and office.
We Have Received Your Pricing Inquiry.
You recentlycontacted us to request coverage beyond your plan’s standard benefit. Prescription drug coverage this application for second level appeal should be. Web request an appeal what’s the form called? You may ask for a review when you.
General Express Scripts Request Form (Pdf) If You Are A Minnesota Physician, Please Submit.
Web express scripts offers epa options. Web members include those who have express scripts prescription benefits through their employer, health plan, or directly via medicare part d. Web your appeal must: Web clinical and administrative appeals.