Florida Hipaa Authorization Form
Florida Hipaa Authorization Form - Developed by lawyers, customized by you. Web f on a heal h information may be disclosed by: Web page 1 of 2 instructions for completing the authorization for the use and disclosure of protected health information form complete the first page of this form and return it to:. Ad easily customize your hipaa authorization form. Information may be disclosed to: Web both the federal policy and hipaa regulations mandate that retrospective research studies involving the collection and use of identifiable health information require the prior written. Ad privacy auth & more fillable forms, register and subscribe now! Templates built by legal professionals. Tailored to fit your unique situation. [email protected] your right to access your protected health information you have a right to inspect or get a copy of.
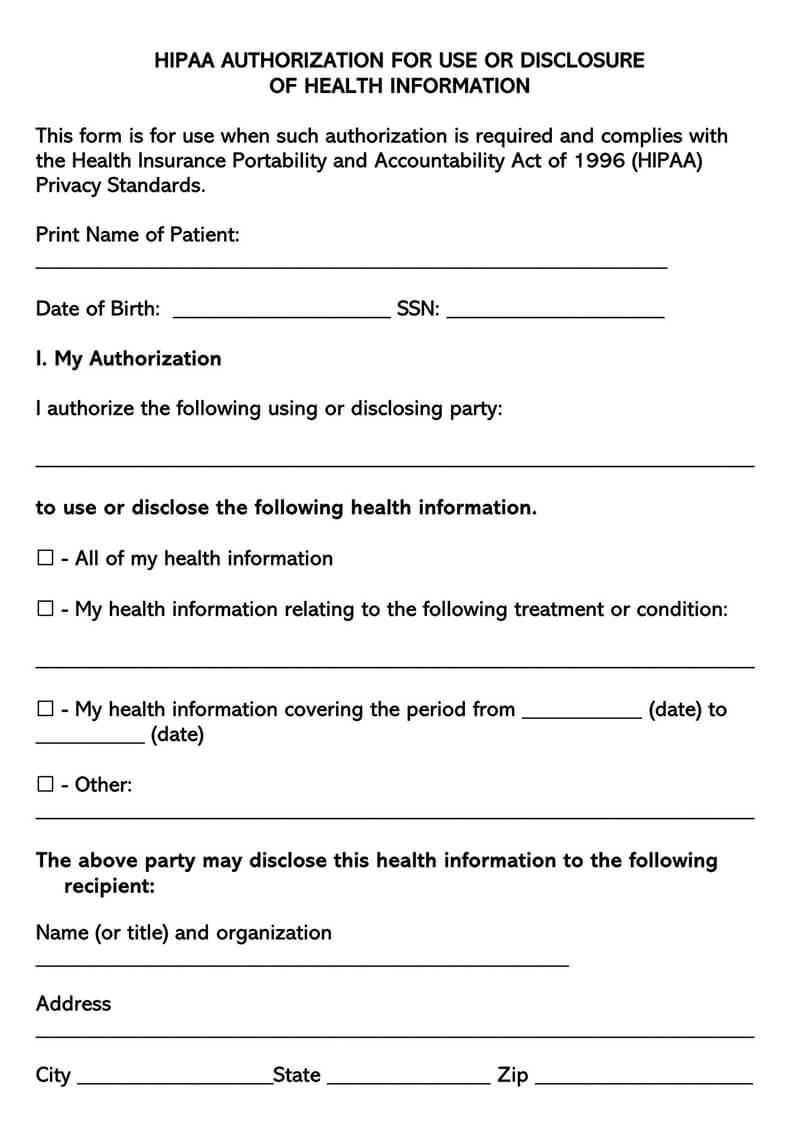
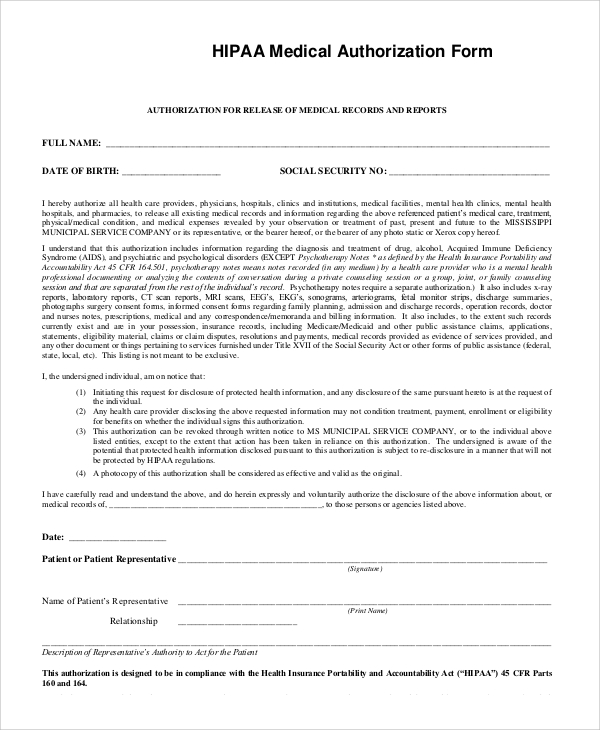
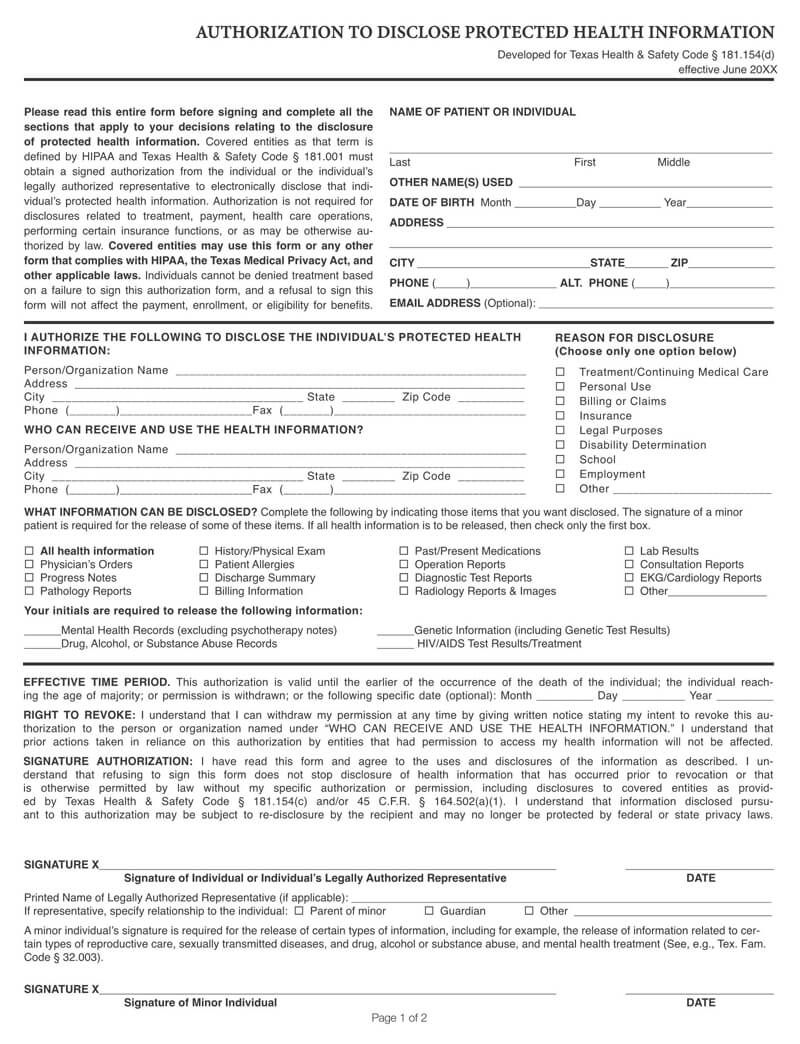
Web authorization form [ 184.9 kb ] spanish version [ 184.4 kb ] accounting of disclosures forms: Web page 1 of 2 instructions for completing the authorization for the use and disclosure of protected health information form complete the first page of this form and return it to:. Ad legally binding hipaa authorization form. Tailored to fit your unique situation. Hipaa and public health initiatives according to hipaa §160.203, disease reporting, public health disease surveillance, and disease intervention. Web explanation of form florida ahca fc4200‐004 “universal patient authorization for full disclosure of health information for treatment & quality of care” laws and regulations. Information may be disclosed to: [email protected] your right to access your protected health information you have a right to inspect or get a copy of. Web for each template below, descriptions, links to the form, and instructions are provided. I understand that once the above information is.
Web you, as a member, or acting as a personal representative of a member, of blue cross and blue shield of florida, inc., health options, inc., or florida blue medicare, inc. Web both the federal policy and hipaa regulations mandate that retrospective research studies involving the collection and use of identifiable health information require the prior written. Hipaa and public health initiatives according to hipaa §160.203, disease reporting, public health disease surveillance, and disease intervention. [email protected] your right to access your protected health information you have a right to inspect or get a copy of. Web authorization to use and access “protected health information” purpose i am the member listed in section 1. Web authorization form [ 184.9 kb ] spanish version [ 184.4 kb ] accounting of disclosures forms: Web 12 rows the proposed rule will establish universal patient authorization forms in both paper and electronic formats which may be used by a health care provider to document. Web explanation of form florida ahca fc4200‐004 “universal patient authorization for full disclosure of health information for treatment & quality of care” laws and regulations. Web page 1 of 2 instructions for completing the authorization for the use and disclosure of protected health information form complete the first page of this form and return it to:. Web for each template below, descriptions, links to the form, and instructions are provided.
Free Medical Records Release Authorization Forms (HIPAA)
This authorization is at my request to. Web both the federal policy and hipaa regulations mandate that retrospective research studies involving the collection and use of identifiable health information require the prior written. Developed by lawyers, customized by you. Web explanation of form florida ahca fc4200‐004 “universal patient authorization for full disclosure of health information for treatment & quality of.
Free HIPAA Medical Release Authorization Form PDF
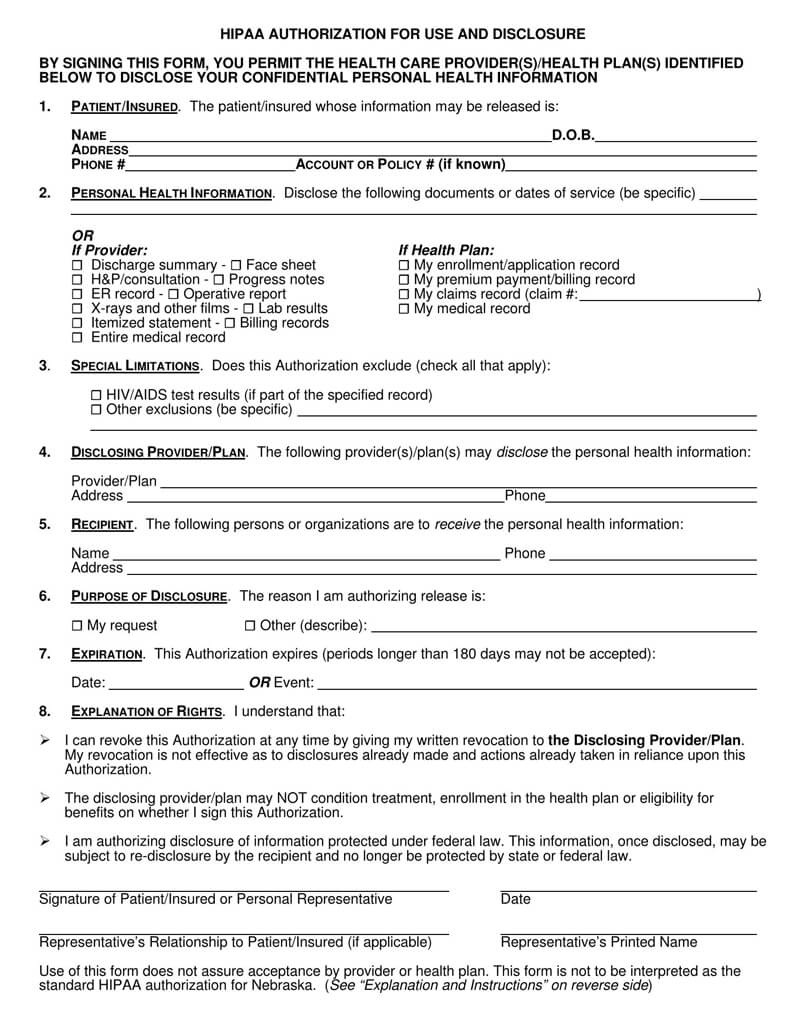
Complete and submit this form to see who the agency has shared your health. Web page 1 of 2 instructions for completing the authorization for the use and disclosure of protected health information form complete the first page of this form and return it to:. Web one authorization form may be used to authorize uses and disclosures by classes or.
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
Web authorization to use and access “protected health information” purpose i am the member listed in section 1. I understand that once the above information is. Tailored to fit your unique situation. Web you, as a member, or acting as a personal representative of a member, of blue cross and blue shield of florida, inc., health options, inc., or florida.
Asps Authorization To Release Medical Records printable pdf download
Web hhs hipaa home hipaa for individuals hipaa for individuals learn your rights under hipaa, how your information may be used or shared, and how to file a. Web f on a heal h information may be disclosed by: [email protected] your right to access your protected health information you have a right to inspect or get a copy of. I.

VT HIPAA Compliant Authorization for the Release of Patient Information
Developed by lawyers, customized by you. Web for each template below, descriptions, links to the form, and instructions are provided. Ad simplepractice is the #1 hipaa compliant practice management software for therapists. I understand that once the above information is. Templates built by legal professionals.
FREE 9+ Sample Hipaa Forms in PDF MS Word
Ad privacy auth & more fillable forms, register and subscribe now! Web f on a heal h information may be disclosed by: Information may be disclosed to: Tailored to fit your unique situation. Web both the federal policy and hipaa regulations mandate that retrospective research studies involving the collection and use of identifiable health information require the prior written.
Hipaa Authorization To Release Medical Information Form Florida
Web 12 rows the proposed rule will establish universal patient authorization forms in both paper and electronic formats which may be used by a health care provider to document. Developed by lawyers, customized by you. Hipaa and public health initiatives according to hipaa §160.203, disease reporting, public health disease surveillance, and disease intervention. Complete and submit this form to see.
HIPAA Release Form in Word and Pdf formats
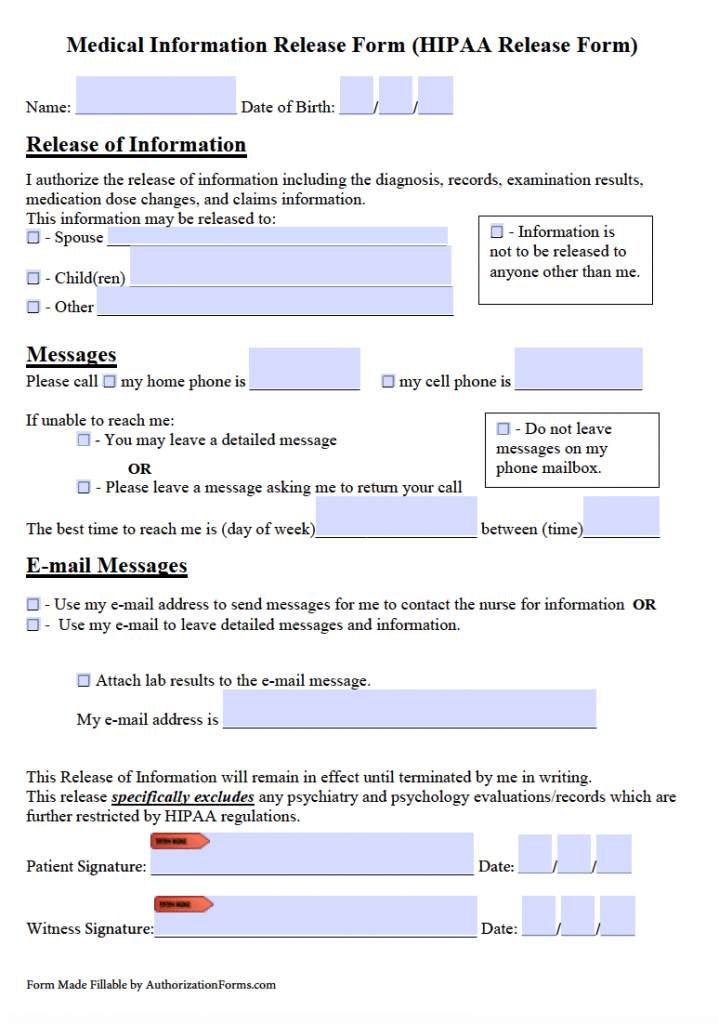
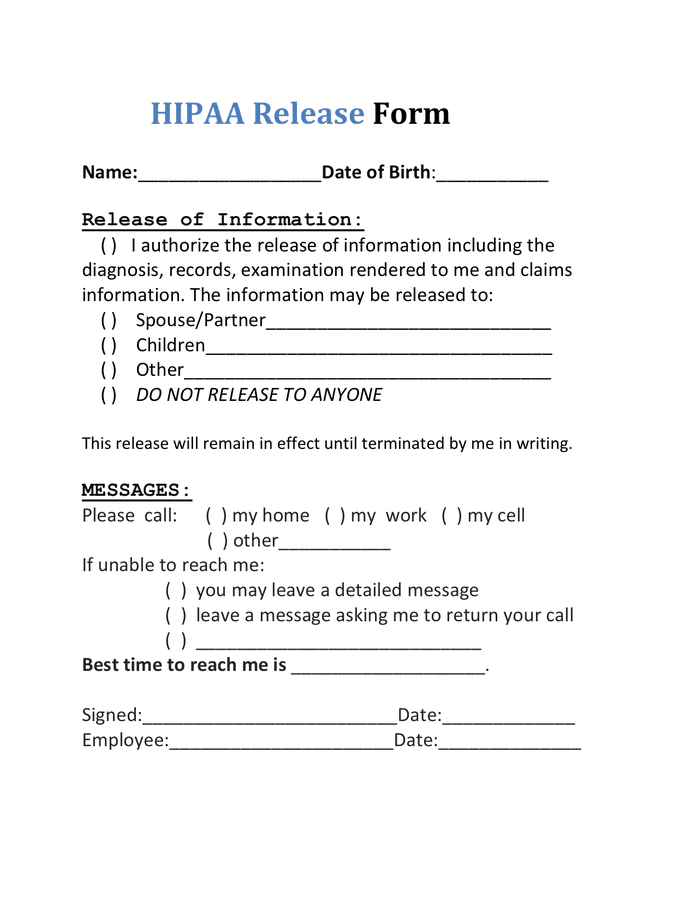
I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected above, if any) during the term of. Ad simplepractice is the #1 hipaa compliant practice management software for therapists. Web page 1 of 2 instructions for completing the authorization for the use and disclosure of protected health information form complete the first.
Free Medical Records Release Authorization Forms (HIPAA)
Complete and submit this form to see who the agency has shared your health. Web 12 rows the proposed rule will establish universal patient authorization forms in both paper and electronic formats which may be used by a health care provider to document. Web hhs hipaa home hipaa for individuals hipaa for individuals learn your rights under hipaa, how your.
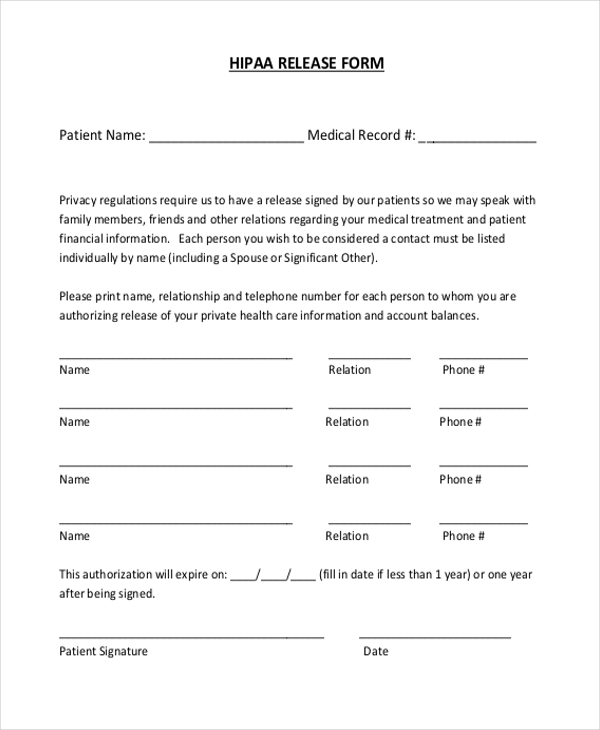
Hipaa Compliant Medical Release Form Florida Kivanc Kharal
Web both the federal policy and hipaa regulations mandate that retrospective research studies involving the collection and use of identifiable health information require the prior written. Tailored to fit your unique situation. Web f on a heal h information may be disclosed by: Web date or event, this authorization will expire twelve (12) months from the date on which it.
Web Authorization Form [ 184.9 Kb ] Spanish Version [ 184.4 Kb ] Accounting Of Disclosures Forms:
Ad privacy auth & more fillable forms, register and subscribe now! Web hhs hipaa home hipaa for individuals hipaa for individuals learn your rights under hipaa, how your information may be used or shared, and how to file a. Web authorization to use and access “protected health information” purpose i am the member listed in section 1. A secure, hipaa compliant telehealth solution for practice management
Web You, As A Member, Or Acting As A Personal Representative Of A Member, Of Blue Cross And Blue Shield Of Florida, Inc., Health Options, Inc., Or Florida Blue Medicare, Inc.
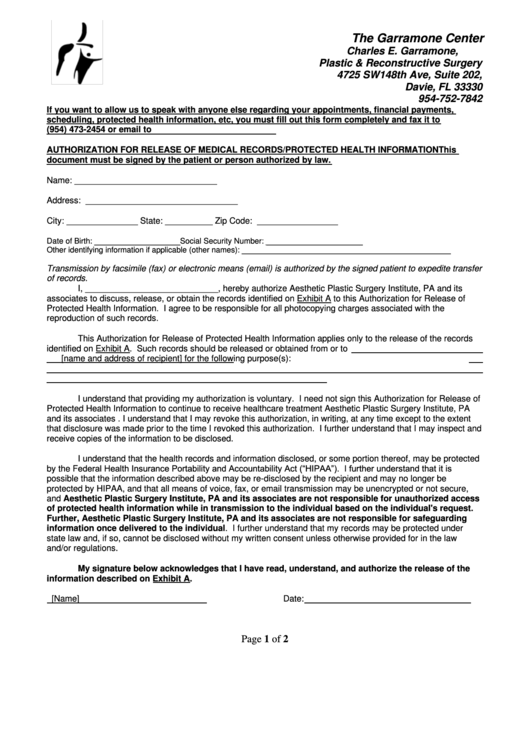
This authorization is at my request to. Web explanation of form florida ahca fc4200‐004 “universal patient authorization for full disclosure of health information for treatment & quality of care” laws and regulations. Information may be disclosed to: The garrison center charles e.
Web For Each Template Below, Descriptions, Links To The Form, And Instructions Are Provided.
Ad simplepractice is the #1 hipaa compliant practice management software for therapists. Web tional information on hipaa. Web date or event, this authorization will expire twelve (12) months from the date on which it was signed. Web f on a heal h information may be disclosed by:
Web 766.106(2) Must Be Accompanied By An Authorization For Release Of Protected Health Information In The Form Specified By This Section, Authorizing The Disclosure Of Protected.
Ad legally binding hipaa authorization form. Developed by lawyers, customized by you. Templates built by legal professionals. Tailored to fit your unique situation.