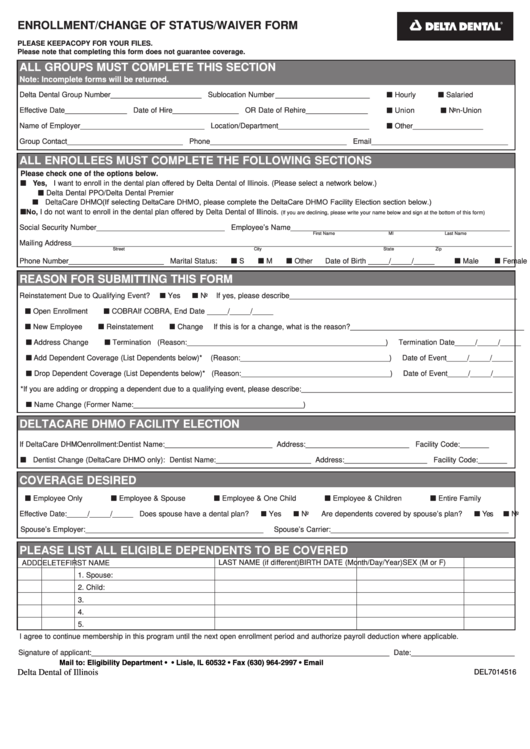
Health And Dental Enrollment Form Purpose
Health And Dental Enrollment Form Purpose - Providers can contact the provider enrollment unit for questions regarding. The provider may access the provider enrollment application and guide for assistance. In the 2 “employer/group city” field, enter your district’s county. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any medical. Authorization for disclosure of protected health information. 2023 top health insurance plans & coverage. Employee information (please print) home phone work phone gender (m/f) marital. If you cannot apply online the next best option is to scan. Our office remains on the edge of the latest technologies used in delivering outstanding dental. Refer to the instructions on the back before completing this form.
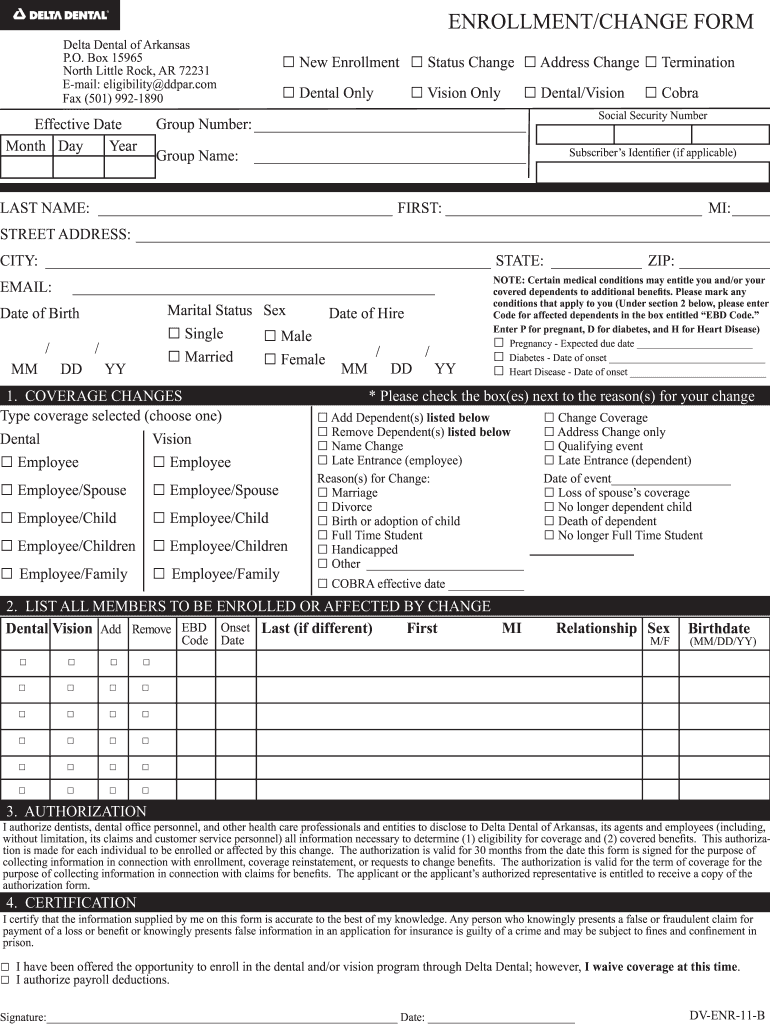
Refer to the instructions on the back before completing this form. • if you are subject to “additional medicare tax”, attach a copy of federal. In the 2 “employer/group city” field, enter your district’s county. Web in all circumstances, the insurance enrollment forms must be signed, dated, and submitted by 30 days after your hire date or you will lose your opportunity to enroll as a new hire. Web dental enrollment/change request aetna life insurance company* instructions: Ad missouri dental insurance plans. Ad affordable insurance plans from top carriers. The enrollment may have been terminated because your annuity was terminated, because you entered military. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Web if you decline health/dental enrollment for yourself and your dependents, a request for enrollment at a later date may not be allowed, or may be subject to late enrollment.
Ad affordable insurance plans from top carriers. Cobra continuation of group dental coverage form. Lump sum distribution (form 4972) recapture of low income housing credit (form 8611) 31. Group health and dental enrollment form. Providers can contact the provider enrollment unit for questions regarding. Web group health and dental enrollment form. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any medical. Start your free online quote. The provider may access the provider enrollment application and guide for assistance. Web if you decline health/dental enrollment for yourself and your dependents, a request for enrollment at a later date may not be allowed, or may be subject to late enrollment.
Top 52 Delta Dental Forms And Templates free to download in PDF format
In the 2 “employer/group city” field, enter your district’s county. The provider may access the provider enrollment application and guide for assistance. Providers can contact the provider enrollment unit for questions regarding. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Web dental enrollment/change request aetna life.

Dental and Vision Enrollment Form Fraud Insurance
Complete the enrollment form below. Web this form is used to reinstate your health benefits enrollment. Cobra continuation of group dental coverage form. Web let’s now take a look at page two of the health benefits enrollment form. Employee information (please print) home phone work phone gender (m/f) marital.

Sun Life Group Benefits Enrolment Form 20202021 Fill and Sign
Start your free online quote. Web group health and dental enrollment form. Plan options that bundle vision and hearing, too. Group health and dental enrollment form. • if you are subject to “additional medicare tax”, attach a copy of federal.
Delta Dental Enrollment Form Fill Out and Sign Printable PDF Template
Please complete all sections, as appropriate. Cobra continuation of group dental coverage form. Web your dental plan enrollment form you can also enroll online at [dentalhealthservices.com] you’re only a few steps away from a healthier and smarter smile! • if you are subject to “additional medicare tax”, attach a copy of federal. Apply using the dss online portal for all.

Metlife Dental Enrollment Form.pdf Google Drive
Web independent health’s 55+ dental plan 1. Providers can contact the provider enrollment unit for questions regarding. Lump sum distribution (form 4972) recapture of low income housing credit (form 8611) 31. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any medical. Group health and.

Altus Dental Enrollment form.pdf Google Drive
Start your free online quote. Providers can contact the provider enrollment unit for questions regarding. Sign and date this form in section 6. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Authorization for disclosure of protected health information.
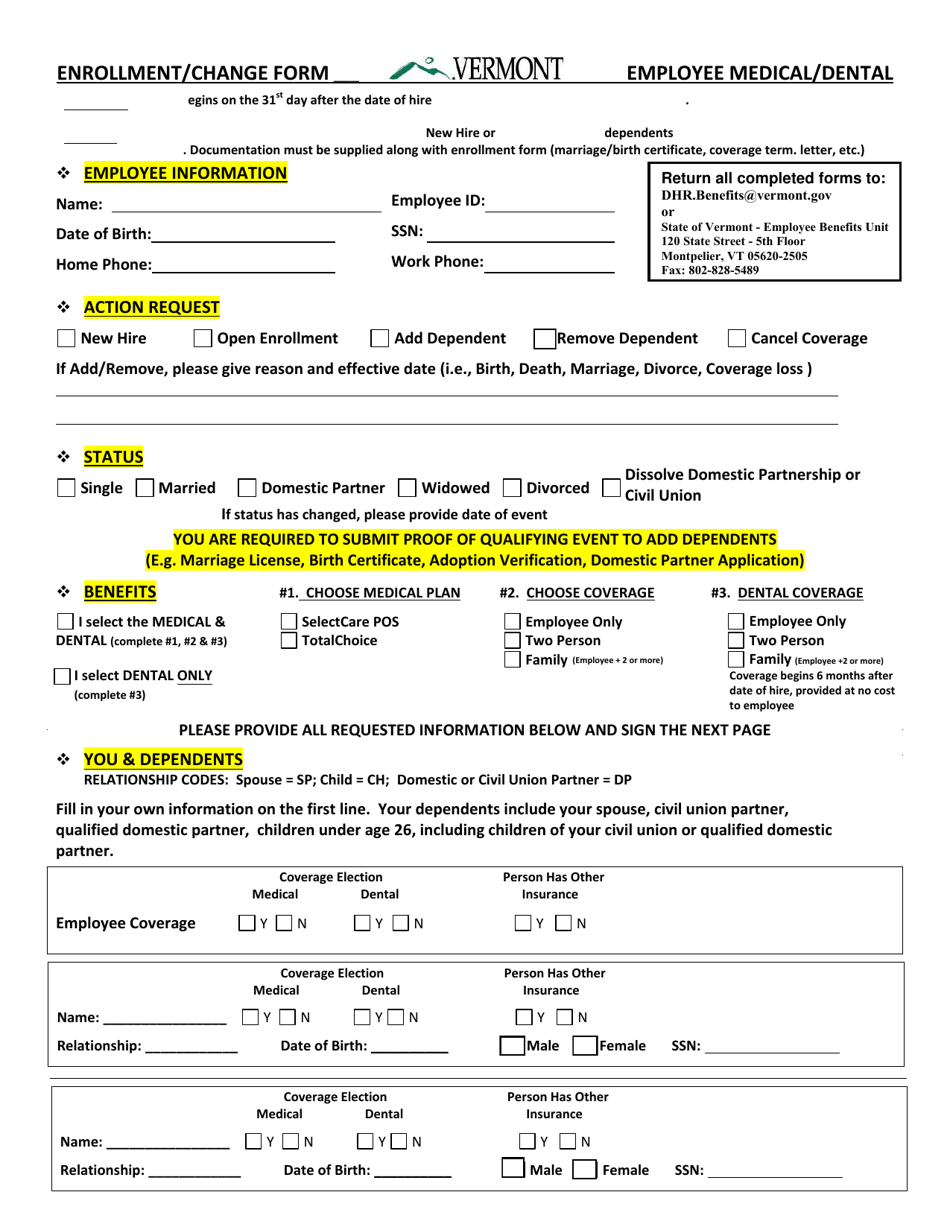
Vermont Medical/Dental Enrollment Form Download Fillable PDF
Lump sum distribution (form 4972) recapture of low income housing credit (form 8611) 31. Authorization for disclosure of protected health information. Web in all circumstances, the insurance enrollment forms must be signed, dated, and submitted by 30 days after your hire date or you will lose your opportunity to enroll as a new hire. Dental coverage from basic to comprehensive..

Oral Health Matters Dental Enrollment Contributes to ACA 1st Year Success
Our office remains on the edge of the latest technologies used in delivering outstanding dental. Ad missouri dental insurance plans. Apply using the dss online portal for all applications. • if you are subject to “additional medicare tax”, attach a copy of federal. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it.

Pin on Dental Nursing NEBDN Diploma Level 3
Ad missouri dental insurance plans. Our office remains on the edge of the latest technologies used in delivering outstanding dental. Providers can contact the provider enrollment unit for questions regarding. Instantly find the best price! Dental coverage from basic to comprehensive.
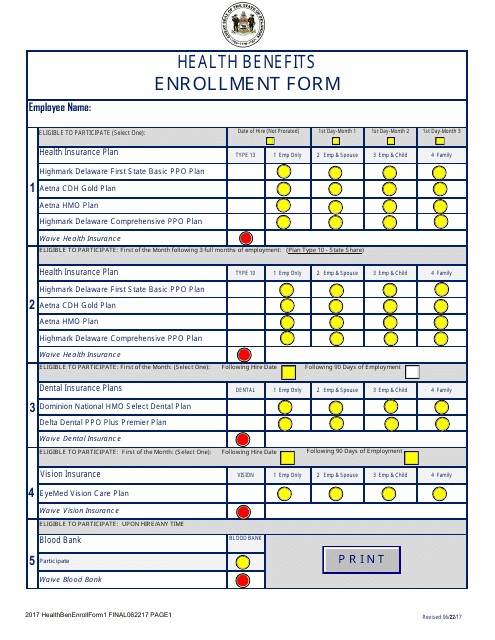
Delaware Health Benefits Enrollment Form Download Fillable PDF
Cobra continuation of group dental coverage form. Web independent health’s 55+ dental plan 1. Ad affordable insurance plans from top carriers. • if you are subject to “additional medicare tax”, attach a copy of federal. Providers can contact the provider enrollment unit for questions regarding.
Be Sure To Complete All The Information Requested On The Form, Including The Type Of.
The provider may access the provider enrollment application and guide for assistance. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any medical. Apply using the dss online portal for all applications. Web group health and dental enrollment form.
Plan Options That Bundle Vision And Hearing, Too.
Start your free online quote. Please complete all sections, as appropriate. Web in all circumstances, the insurance enrollment forms must be signed, dated, and submitted by 30 days after your hire date or you will lose your opportunity to enroll as a new hire. Web missouri now uses a single application form to apply for medicaid.
Sign And Date This Form In Section 6.
Web this form is used to reinstate your health benefits enrollment. Cobra continuation of group dental coverage form. Web hermann family dental is committed to giving you the smile of your dreams. Web independent health’s 55+ dental plan 1.
If You Chose To Participate In A Health Or Dental Plan, You Will Now Need To Complete This Section Of The.
Group health and dental enrollment form. If you cannot apply online the next best option is to scan. The enrollment may have been terminated because your annuity was terminated, because you entered military. • if you are subject to “additional medicare tax”, attach a copy of federal.