Molina Credentialing Form
Molina Credentialing Form - In accordance with those standards,. The practitioner must sign and date their. Providers date of birth (mm/dd/yy): Pick your state and your preferred language to continue. Practitioner application instructions complete all items as noted below and submit this application and attachments to your contracting. Last four digits of ss#: By submitting my information via this form, i. Is listed as an authorized plan to view your credentialing application caqh id #: Web credentialing molina healthcare has a duty to protect its members by assuring the care they receive is of the highest quality. Web molina healthcare of ohio’s credentialing process is designed to meet the standards of the national committee for quality assurance (ncqa).
To join molina healthcare of mississippi's mississippican (medicaid) network, from july 1, 2022, you must be credentialed by the mississippi division of medicaid and. Web credentialing molina healthcare has a duty to protect its members by assuring the care they receive is of the highest quality. Practitioner application instructions complete all items as noted below and submit this application and attachments to your contracting. Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa. Web molina requirements for credentialing: Pick your state and your preferred language to continue. Web credentialing contact (if different from above): Web the behavioral health special provider bulletin is a newsletter distributed by molina healthcare of ohio. The practitioner must sign and date their. Prior authorization request contact information.
Receive notification of your rights as a provider to appeal. Web the behavioral health special provider bulletin is a newsletter distributed by molina healthcare of ohio. Receive notification of the credentialing decision within 60 days of the committee decision; ( ) name affiliated with tax id number: By submitting my information via this form, i. Web ensure molina healthcare, inc. In accordance with those standards,. Last four digits of ss#: Web credentialing contact (if different from above): Pick your state and your preferred language to continue.
Aetna Better Health Prior Authorization Fill and Sign Printable
• a completed credentialing application, which includes but is not limited to: Web molina requirements for credentialing: By submitting my information via this form, i. Web the behavioral health special provider bulletin is a newsletter distributed by molina healthcare of ohio. Pick your state and your preferred language to continue.
Credentialing Request Form Fill Out and Sign Printable PDF Template
In accordance with those standards,. One protection is assurance that. Practitioner application instructions complete all items as noted below and submit this application and attachments to your contracting. Receive notification of your rights as a provider to appeal. Web molina requirements for credentialing:
Molina Healthcare Credentialing Forms Form Resume Examples xz20pnnx2q
Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa. • a completed credentialing application, which includes but is not limited to: Web ensure molina healthcare, inc. Receive notification of your rights as a provider to appeal. Providers date of birth (mm/dd/yy):

Form Standardized Credentialing Fill Online, Printable, Fillable
( ) name affiliated with tax id number: Web credentialing contact (if different from above): Web molina healthcare of ohio’s credentialing process is designed to meet the standards of the national committee for quality assurance (ncqa). Web find out if you can become a member of the molina family. Receive notification of the credentialing decision within 60 days of the.
20012021 MO Standardized Credentialing Form Fill Online, Printable
The practitioner must sign and date their. Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa. Web molina healthcare of ohio’s credentialing process is designed to meet the standards of the national committee for quality assurance (ncqa). Web molina requirements for credentialing: By submitting my information via this.
Molina Healthcare Credentialing Forms Form Resume Examples xz20pnnx2q
Web pharmacy credentialing/recredentialing application completed forms can be sent to: Last four digits of ss#: Web credentialing molina healthcare has a duty to protect its members by assuring the care they receive is of the highest quality. One protection is assurance that. To join molina healthcare of mississippi's mississippican (medicaid) network, from july 1, 2022, you must be credentialed by.
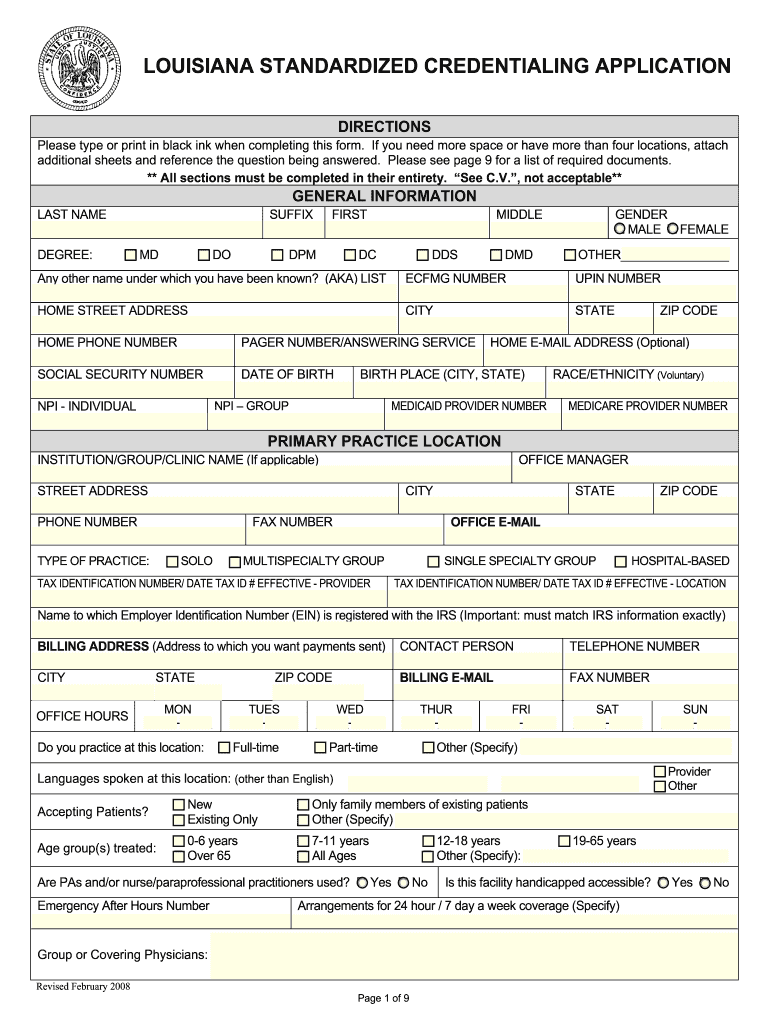
Louisiana Standardized Credentialing Application Fill Out and Sign
Prior authorization request contact information. Pick your state and your preferred language to continue. Web credentialing contact (if different from above): Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa. Web credentialing molina healthcare has a duty to protect its members by assuring the care they receive is.
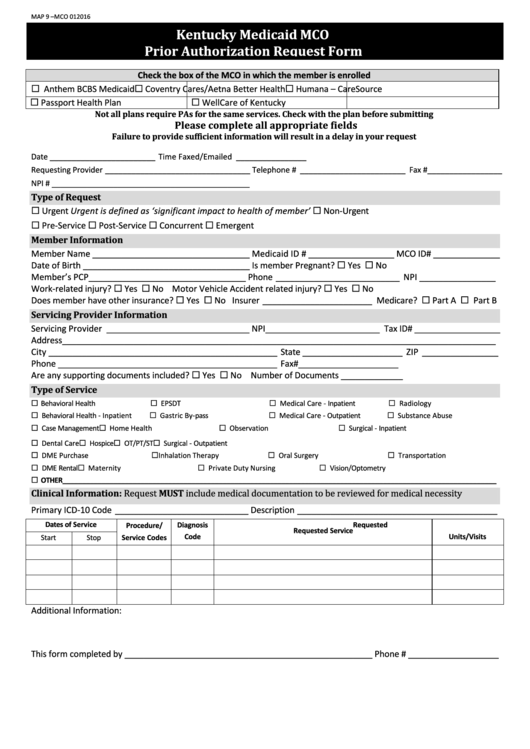
Fillable Kentucky Medicaid Mco Prior Authorization Request Form
Web pharmacy credentialing/recredentialing application completed forms can be sent to: In accordance with those standards,. Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa. Web ensure molina healthcare, inc. Is listed as an authorized plan to view your credentialing application caqh id #:
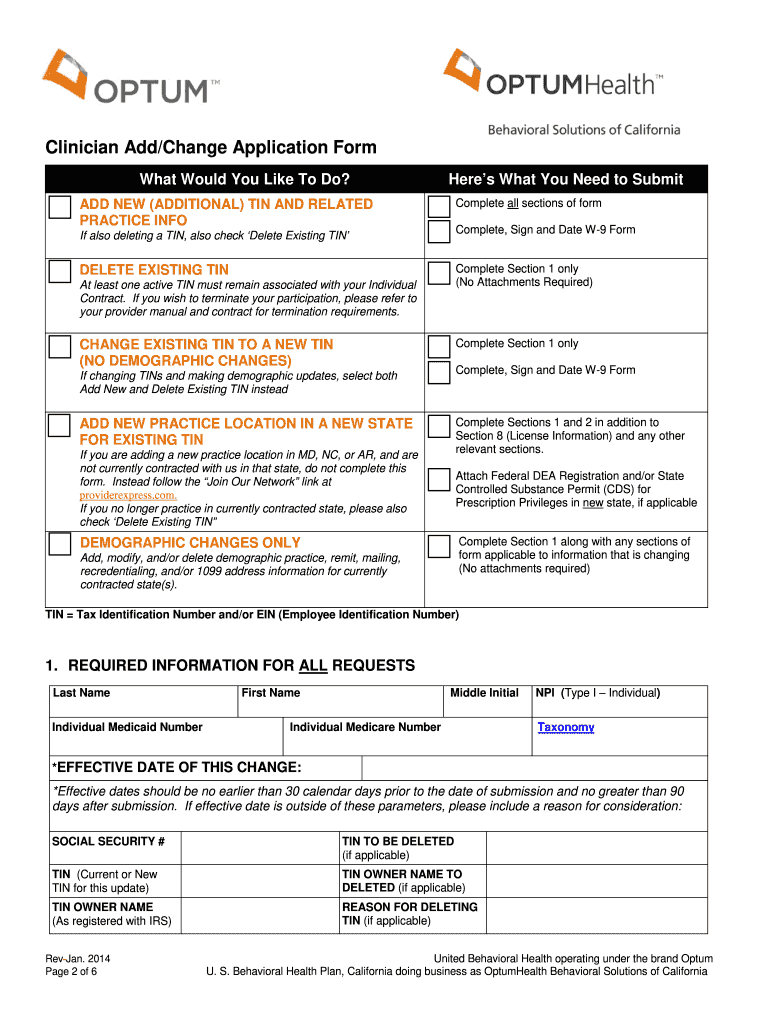
CA Clinician Add/Change Application Form 2014 Fill and Sign Printable
Is listed as an authorized plan to view your credentialing application caqh id #: Web credentialing molina healthcare has a duty to protect its members by assuring the care they receive is of the highest quality. Prior authorization request contact information. Practitioner must complete and submit to molina a credentialing application. Receive notification of your rights as a provider to.
Molina Healthcare Credentialing Forms Form Resume Examples xz20pnnx2q
Receive notification of your rights as a provider to appeal. The application must be entirely complete. Prior authorization request contact information. Web the behavioral health special provider bulletin is a newsletter distributed by molina healthcare of ohio. Pick your state and your preferred language to continue.
Web Credentialing Molina Healthcare Has A Duty To Protect Its Members By Assuring The Care They Receive Is Of The Highest Quality.
The application must be entirely complete. In accordance with those standards,. Is listed as an authorized plan to view your credentialing application caqh id #: One protection is assurance that.
• A Completed Credentialing Application, Which Includes But Is Not Limited To:
To avoid delays please ensure applications are current, including work. By submitting my information via this form, i. Practitioner must complete and submit to molina a credentialing application. Web find out if you can become a member of the molina family.
Web Pharmacy Credentialing/Recredentialing Application Completed Forms Can Be Sent To:
Last four digits of ss#: Providers date of birth (mm/dd/yy): Pick your state and your preferred language to continue. Web washington law requires all health care providers submit credentialing applications through providersource.
Prior Authorization Request Contact Information.
Receive notification of the credentialing decision within 60 days of the committee decision; Web credentialing contact (if different from above): Receive notification of your rights as a provider to appeal. Web molina healthcare prior authorization request form and instructions nursing facility request form synagis (rsv) authorization behavioral health respite services pa.