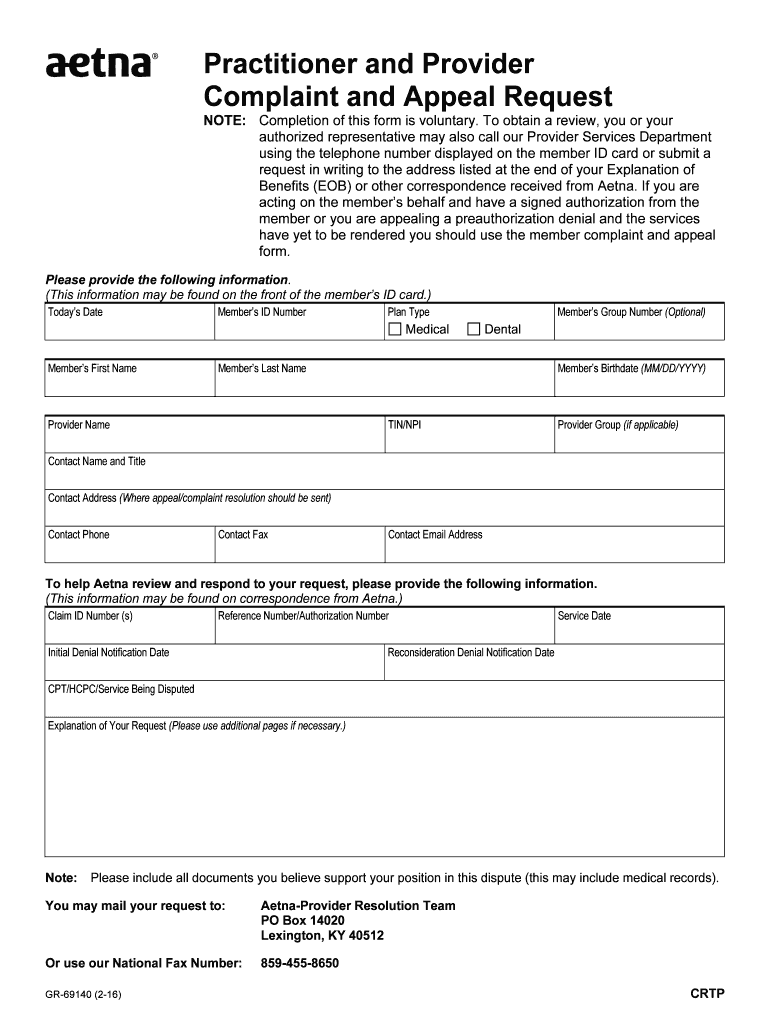
Provider Complaint And Appeal Form Aetna
Provider Complaint And Appeal Form Aetna - Web form for filing an appeal, formal complaint or suggestion. Or use our national fax number: Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. You must complete this form. Get a medicare provider complaint and appeal form (pdf) get a provider complaint. We’re here to make filing a complaint a little easier. Web medicare provider complaint and appeal request note: Web what if i use the provider complaint and appeal form to submit a reconsideration? To obtain a review, you’ll need to submit this form. Do i need to resubmit all information on an appeal that was submitted on the reconsideration?
Web form for filing an appeal, formal complaint or suggestion. We’re here to make filing a complaint a little easier. Web what if i use the provider complaint and appeal form to submit a reconsideration? Do i need to resubmit all information on an appeal that was submitted on the reconsideration? Web complaint and appeal form. Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. To obtain a review, you’ll need to submit this form. Make sure to include any information that will support your appeal. You must complete this form. This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member.
This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member. To obtain a review, you’ll need to submit this form. To obtain a review, you’ll need to submit this form. Or use our national fax number: You must complete this form. What if i submit a reconsideration that is actually an appeal? How can i tell if the response i received was handled as a reconsideration or an appeal? Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Web complaint and appeal form. Web form for filing an appeal, formal complaint or suggestion.

AETNA FAIL Here is the rejection letter from Aetna, my appeal, and the
This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member. Aetna better health of michigan attn: Web form for filing an appeal, formal complaint or suggestion. Web.
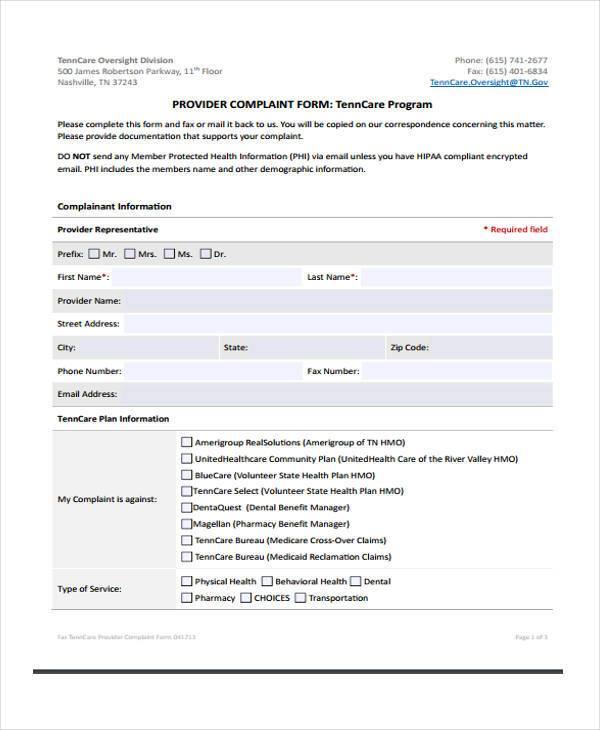
FREE 9+ Medicare Complaint Forms in PDF MS Word
Web form for filing an appeal, formal complaint or suggestion. We’re here to make filing a complaint a little easier. You must complete this form. Grievance & appeals po box 81040 cleveland, oh 44181. Web what if i use the provider complaint and appeal form to submit a reconsideration?
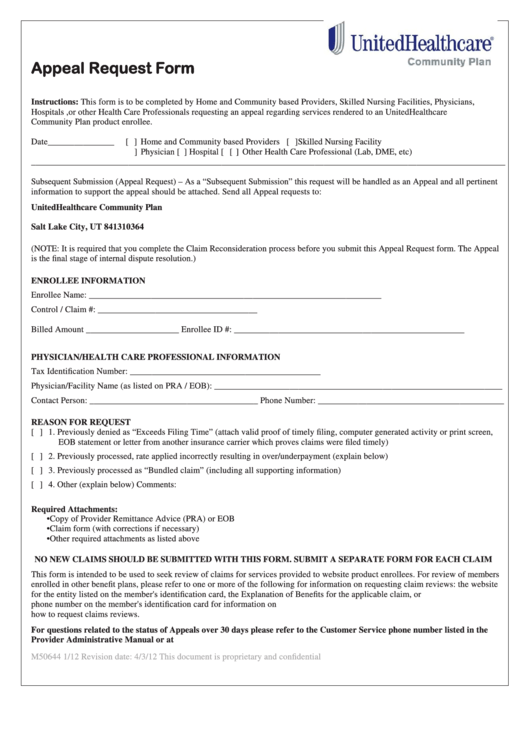
Top United Healthcare Appeal Form Templates free to download in PDF format
Grievance & appeals po box 81040 cleveland, oh 44181. To obtain a review, you’ll need to submit this form. You must complete this form. Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. This form is.
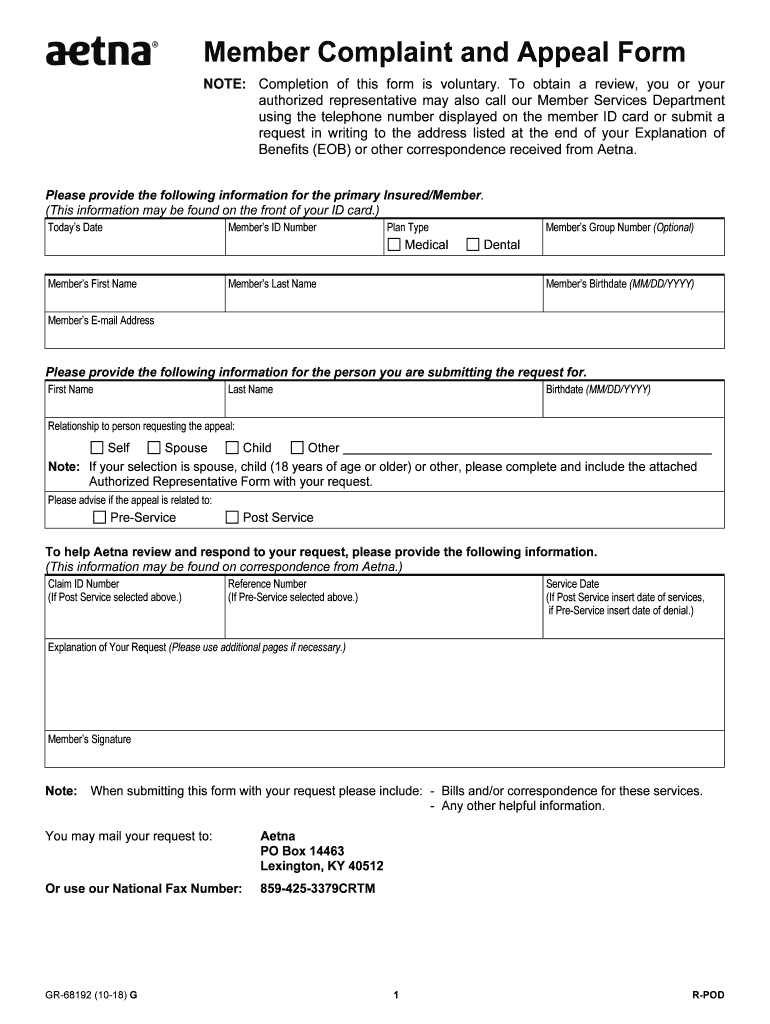
20182021 Form Aetna GR68192 Fill Online, Printable, Fillable, Blank
Get a medicare provider complaint and appeal form (pdf) get a provider complaint. This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member. Web what if i.

Appeal Insurance Claim Denial Letter Sample aesthetic name
To obtain a review, you’ll need to submit this form. Make sure to include any information that will support your appeal. Grievance & appeals po box 81040 cleveland, oh 44181. Web medicare provider complaint and appeal request note: This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna.
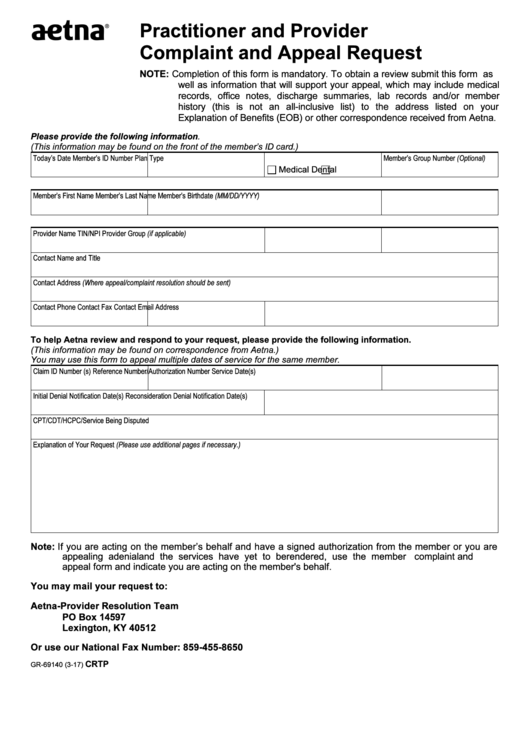
Fillable Form Gr69140 Aetna Practitioner And Provider Complaint And
To obtain a review, you’ll need to submit this form. Get a medicare provider complaint and appeal form (pdf) get a provider complaint. How can i tell if the response i received was handled as a reconsideration or an appeal? These changes do not affect member appeals. Or use our national fax number:
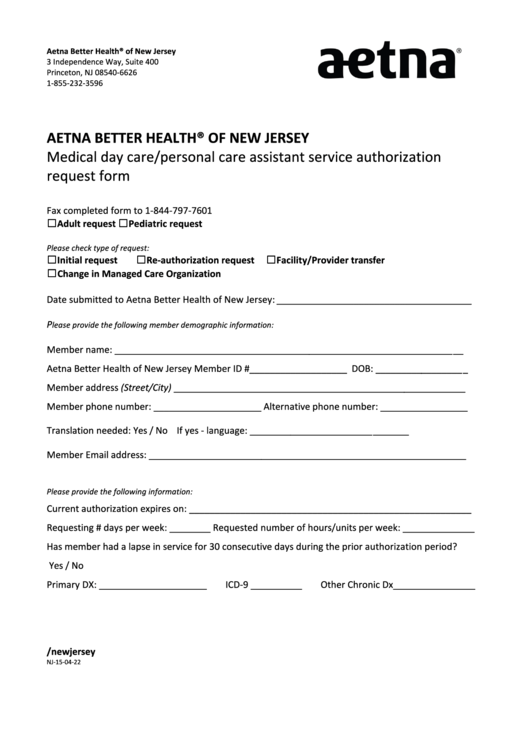
Aetna Better Health Form Of New Jersey printable pdf download
Web form for filing an appeal, formal complaint or suggestion. Web what if i use the provider complaint and appeal form to submit a reconsideration? How can i tell if the response i received was handled as a reconsideration or an appeal? Web 3 ways to file a complaint you have the right to make your voice heard about your.
Aetna Appeal Form 20202022 Fill and Sign Printable Template Online
You may mail your request to: Web complaint and appeal form. This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member. Web form for filing an appeal,.
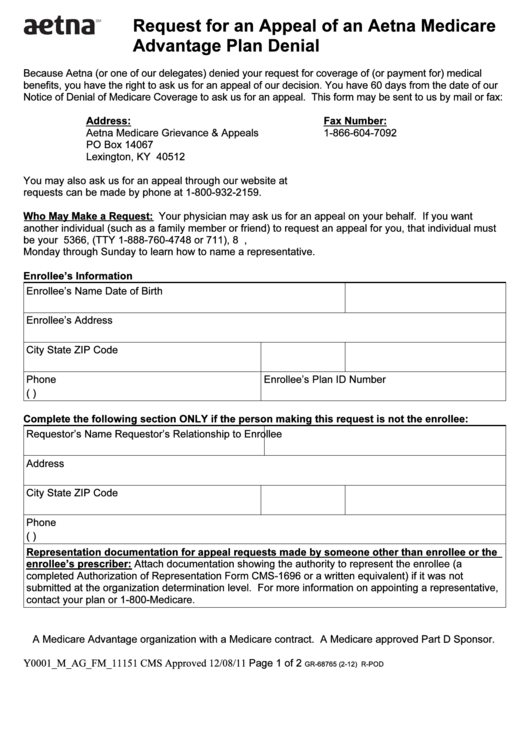
Fillable Form Gr68765 (212) Request For An Appeal Of An Aetna
Grievance & appeals po box 81040 cleveland, oh 44181. Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. We’re here to make filing.
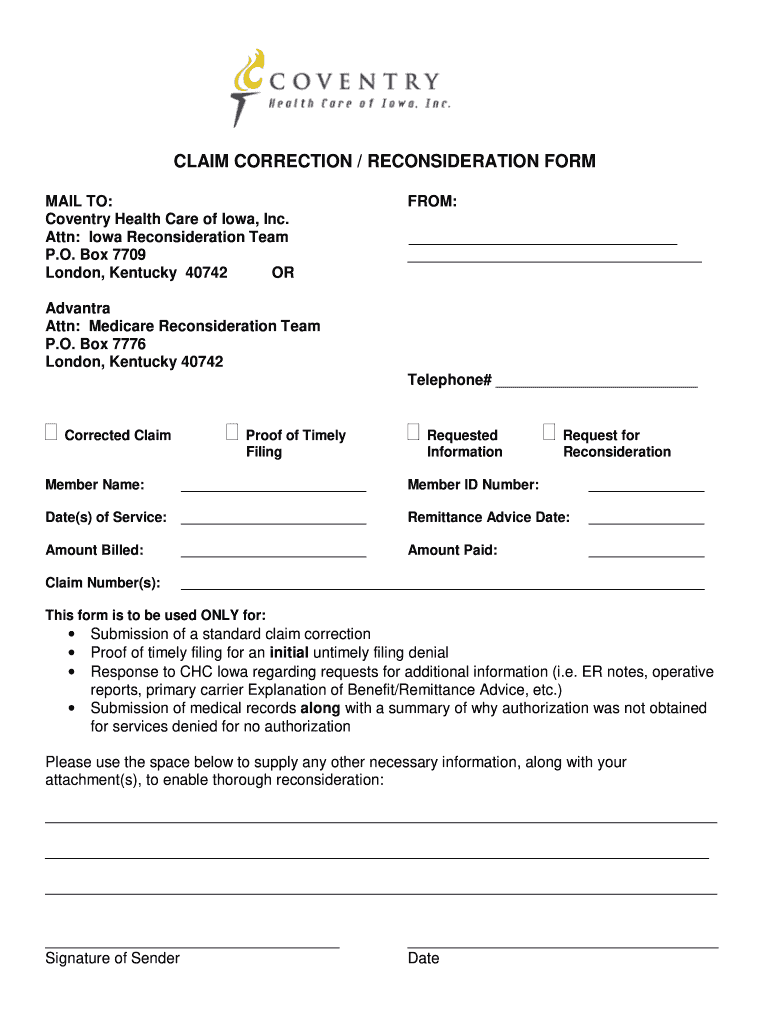
Aetna Reconsideration Form Fill Out and Sign Printable PDF Template
Grievance & appeals po box 81040 cleveland, oh 44181. Web form for filing an appeal, formal complaint or suggestion. Get a medicare provider complaint and appeal form (pdf) get a provider complaint. Web complaint and appeal form. Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna.
What If I Submit A Reconsideration That Is Actually An Appeal?
You must complete this form. Web form for filing an appeal, formal complaint or suggestion. Do i need to resubmit all information on an appeal that was submitted on the reconsideration? You may mail your request to:
Web Medicare Provider Complaint And Appeal Request Note:
How can i tell if the response i received was handled as a reconsideration or an appeal? Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Web what if i use the provider complaint and appeal form to submit a reconsideration? Or use our national fax number:
Grievance & Appeals Po Box 81040 Cleveland, Oh 44181.
Get a medicare provider complaint and appeal form (pdf) get a provider complaint. These changes do not affect member appeals. Web complaint and appeal form. Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider.
We’re Here To Make Filing A Complaint A Little Easier.
Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. This form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member. To obtain a review, you’ll need to submit this form. Make sure to include any information that will support your appeal.