Unitedhealthcare Reconsideration Form
Unitedhealthcare Reconsideration Form - Web this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Unitedhealthcare complaint and appeals department p.o. Box 25183 santa ana, ca 92799. Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10: An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or. Optumrx prior authorization department p.o. Web an appeal is a request for a formal review of an adverse benefit decision. Easily fill out pdf blank, edit, and sign. Wolff, kimberly a created date: Find reconsideration form for uhc and click on get form to get started.
Web step 1 is to file a claim reconsideration request. To file an appeal in writing, please complete the medicare plan. Optumrx prior authorization department p.o. Web how to edit and esign unitedhealthcare reconsideration request form without breaking a sweat. Easily fill out pdf blank, edit, and sign them. Web an appeal is a request for a formal review of an adverse benefit decision. Easily fill out pdf blank, edit, and sign them. Easily fill out pdf blank, edit, and sign. Unitedhealthcare complaint and appeals department p.o. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact.
Web because we, unitedhealthcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Web part c grievances unitedhealthcare community plan. The request must include the claim reconsideration form located on uhcprovider.com/claims > submit a claim reconsideration and all. Easily sign the united healthcare provider appeal form 2022 with your finger. Web an appeal may be filed in writing or by contacting unitedhealthcare customer service. To file an appeal in writing, please complete the medicare plan. Web get the united healthcare reconsideration form you want. Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. Easily fill out pdf blank, edit, and sign. • please submit a separate form for.
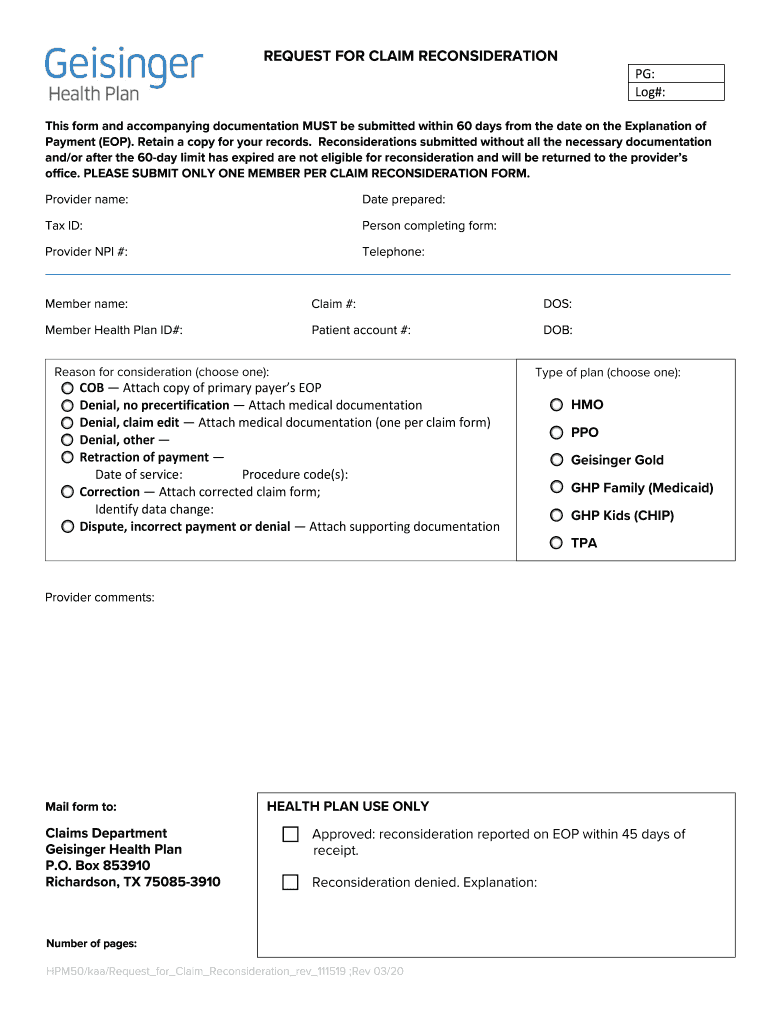
Po Box 853910 Richardson Tx 75085 Fill Out and Sign Printable PDF
Web if you are unable to use the online reconsideration and appeals process outlined in chapter 10: Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact. Web because we, unitedhealthcare, denied your.
Kaiser Senior Advantage Plus Disenrollment Form Form Resume
Web an appeal is a request for a formal review of an adverse benefit decision. Easily fill out pdf blank, edit, and sign them. Web get the united healthcare reconsideration form you want. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact. Step 2 is to file an appeal if you disagree with.
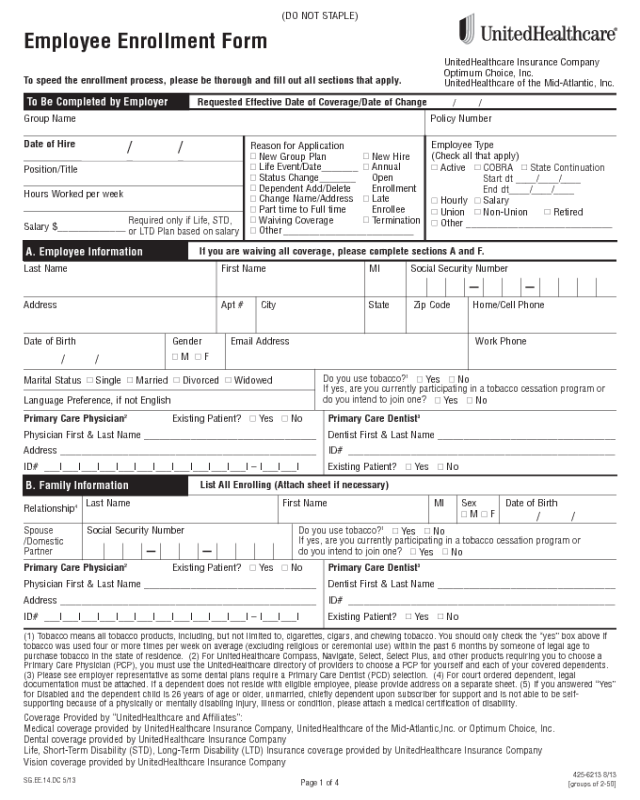
UnitedHealthcare Application Form Edit, Fill, Sign Online Handypdf
Find reconsideration form for uhc and click on get form to get started. Web view and download claim forms by following the link to the global resources portal opens in new window and clicking on my claims. • please submit a separate form for. Web how to edit and esign unitedhealthcare reconsideration request form without breaking a sweat. Open the.

United Care Form Fill Online, Printable, Fillable, Blank pdfFiller
To file an appeal in writing, please complete the medicare plan. The request must include the claim reconsideration form located on uhcprovider.com/claims > submit a claim reconsideration and all. Easily fill out pdf blank, edit, and sign them. • please submit a separate form for. Web if you are unable to use the online reconsideration and appeals process outlined in.

(PDF) UnitedHealthcare Community Plan Claim Reconsideration · PDF
An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or. Web an appeal is a request for a formal review of an adverse benefit decision. Our claims process, mail or fax appeal forms to: Web view and download claim forms by following the link to the global resources portal opens in new.
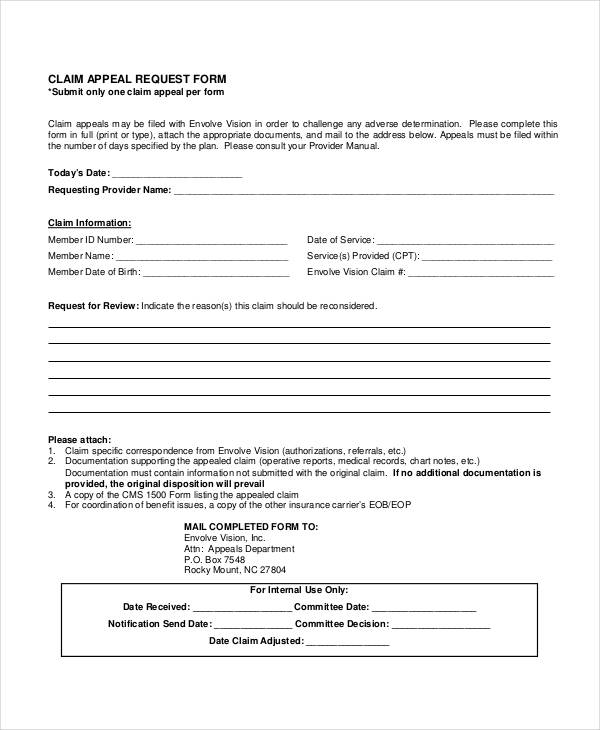
FREE 40+ Claim Forms in PDF Excel MS Word
Open the united healthcare reconsideration form and follow the instructions. • please submit a separate form for. Easily fill out pdf blank, edit, and sign them. Wolff, kimberly a created date: Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more.
2012 Form UnitedHealthcare Waiver of Liability Statement Fill Online
Web step 1 is to file a claim reconsideration request. Wolff, kimberly a created date: Web how to edit and esign unitedhealthcare reconsideration request form without breaking a sweat. Web download the form below and mail or fax it to unitedhealthcare: Step 2 is to file an appeal if you disagree with the outcome of the claim reconsideration decision.
Fillable Medicare Reconsideration Request Form 2nd Level Of Appeal
Web complete this form to request a formulary exception, tiering exception, prior authorization or reimbursement. Web how to edit and esign unitedhealthcare reconsideration request form without breaking a sweat. Web an appeal may be filed in writing or by contacting unitedhealthcare customer service. Find reconsideration form for uhc and click on get form to get started. Web this form is.
Texas Bcbs Provider Appeal Fill Out and Sign Printable PDF Template
Easily fill out pdf blank, edit, and sign them. Easily fill out pdf blank, edit, and sign. Easily fill out pdf blank, edit, and sign them. Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. Web this form is to be completed by physicians, hospitals or other.
Unitedhealthcare Community Plan Ny Dental
Web how to edit and esign unitedhealthcare reconsideration request form without breaking a sweat. An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or. Wolff, kimberly a created date: Web complete this form to request a formulary exception, tiering exception, prior authorization or reimbursement. The following links provide information including, but not.
Fill Out The Blank Fields;
Web this form is to be completed by physicians, hospitals or other health care professionals for claim reconsideration requests for our members. Wolff, kimberly a created date: Optumrx prior authorization department p.o. An adverse benefit decision is a determination about your benefits which results in a denial of service(s), or.
Our Claims Process, Mail Or Fax Appeal Forms To:
Web care provider administrative guides and manuals. Web the unitedhealthcare provider portal allows you to submit referrals, prior authorizations, claims, claim reconsideration and appeals, demographic changes and more. Web because we, unitedhealthcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Web an appeal is a request for a formal review of an adverse benefit decision.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Open the united healthcare reconsideration form and follow the instructions. Easily fill out pdf blank, edit, and sign. Web get the united healthcare reconsideration form you want. The request must include the claim reconsideration form located on uhcprovider.com/claims > submit a claim reconsideration and all.
Box 25183 Santa Ana, Ca 92799.
To file an appeal in writing, please complete the medicare plan. Web here are some commonly used forms you can download to make it quicker to take action on claims, reimbursements and more. Web view and download claim forms by following the link to the global resources portal opens in new window and clicking on my claims. Save or instantly send your.