Wellcare Provider Reconsideration Form
Wellcare Provider Reconsideration Form - Our nurses will give you answers to your medical. Wellcare by allwell member reimbursement department • p.o. Thank you in advance for your. Web disputes, reconsiderations and grievances. Please submit one form per member. Web disputes, reconsiderations and grievances. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Edit, sign, and share wellcare outpatient authorization request form. Ad find a wellcare medicare advantage plan with dental, vision, or hearing. Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state.
Thank you in advance for your. Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Web please select a form from the options below: Web form and required documents to: Wellcare participating provider reconsideration request form. Web disputes, reconsiderations and grievances. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Our nurses will give you answers to your medical. Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state. All fields are required information a request for reconsideration.
Our nurses will give you answers to your medical. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web disputes, reconsiderations and grievances. Outpatient prior authorization form (pdf) inpatient prior certification enter (pdf). Wellcare participating provider reconsideration request form. Please submit one form per member. Ad find a wellcare medicare advantage plan with dental, vision, or hearing. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state. Thank you in advance for your.
Careplus Referral Request Form 20132022 Fill Out and Sign Printable
Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Outpatient prior authorization form (pdf) inpatient prior certification enter (pdf). Web please review the following medicare advantage & prescription drug regulations and guidance reminders regarding sales and enrollment. Our nurses will give you answers to your medical. Web eastpointe and wellcare of.
Wellcare Appeal Form Fill Out and Sign Printable PDF Template signNow
Please submit one form per member. Ad find a wellcare medicare advantage plan with dental, vision, or hearing. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Web wellcare prior authorization form pdf. Web disputes, reconsiderations and grievances.
Virginia Provider Claim Reconsideration Form printable pdf download
Web here are the ways you may request a coverage decision and/or exception. Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state. Wellcare by allwell member reimbursement department • p.o. Web please select a form from the options below: Web form and required documents to:
Wellcare Forms For Prior Authorization Fill Out and Sign Printable
Please submit one form per member. Web please select a form from the options below: Wellcare by allwell member reimbursement department • p.o. Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Web disputes, reconsiderations and grievances.

Wellcare Card 1 newacropol
Web adding new provider to existing contract (pdf) appointment of representative (pdf) delivery notification (pdf) epsdt well child exam form (pdf) epsdt well child. Thank you in advance for your. Web form and required documents to: Web disputes, reconsiderations and grievances. Edit, sign, and share wellcare outpatient authorization request form.
Aarp Printable Application Pdf Fill Online, Printable, Fillable
Web disputes, reconsiderations and grievances. Web adding new provider to existing contract (pdf) appointment of representative (pdf) delivery notification (pdf) epsdt well child exam form (pdf) epsdt well child. Provider dispute form (dates of services 3/31/22 and before) effective april 1, 2022, the following forms should be. Web use this form as part of the wellcare by allwell request for.
Fillable Medicare Reconsideration Request Form 2nd Level Of Appeal
Web please select a form from the options below: Wellcare by allwell member reimbursement department • p.o. Web provider request for reconsideration and claim dispute form use this form as part of the wellcare by allwell request for reconsideration and claim dispute. Please submit one form per member. Web a repository of medicare forms and documents for wellcare providers, covering.
Free WellCare Prior (Rx) Authorization Form PDF eForms
Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Our nurses will give you answers to your medical. Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state. Web please select a form from the options below: Please submit one.
Wellcare Credentialing Application Form Fill Online, Printable
Wellcare by allwell member reimbursement department • p.o. Web please select a form from the options below: Web request for reconsideration and claim dispute form use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and.
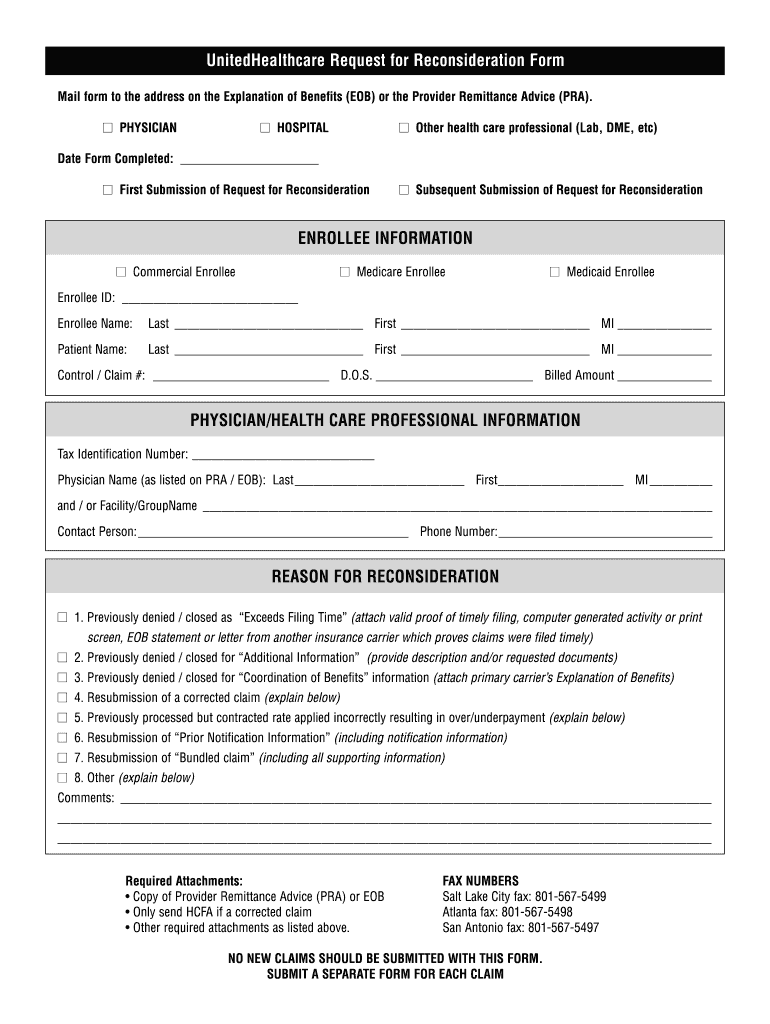
Fillable Online UHC Request For Reconsideration Form Cat Health
Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. >>complete your attestation today!<< access key forms. Wellcare participating provider reconsideration request form. Web adding new provider to existing contract (pdf) appointment of representative (pdf) delivery notification (pdf) epsdt well child exam form (pdf) epsdt well child. Web disputes, reconsiderations and grievances.
Web Provider Request For Reconsideration And Claim Dispute Form Use This Form As Part Of The Wellcare By Allwell Request For Reconsideration And Claim Dispute.
Web request for reconsideration and claim dispute form use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Edit, sign, and share wellcare outpatient authorization request form. Web form and required documents to:
Web Please Review The Following Medicare Advantage & Prescription Drug Regulations And Guidance Reminders Regarding Sales And Enrollment.
Web eastpointe and wellcare of north carolina have local experience managing a robust, comprehensive medicaid network in the state. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Please submit one form per member. Wellcare by allwell member reimbursement department • p.o.
>>Complete Your Attestation Today!<< Access Key Forms.
Thank you in advance for your. Outpatient prior authorization form (pdf) inpatient prior certification enter (pdf). Web disputes, reconsiderations and grievances. Web please select a form from the options below:
Web Adding New Provider To Existing Contract (Pdf) Appointment Of Representative (Pdf) Delivery Notification (Pdf) Epsdt Well Child Exam Form (Pdf) Epsdt Well Child.
Web here are the ways you may request a coverage decision and/or exception. All fields are required information a request for reconsideration. Wellcare participating provider reconsideration request form. Our nurses will give you answers to your medical.