Completed Cms-1500 Form Sample 2020
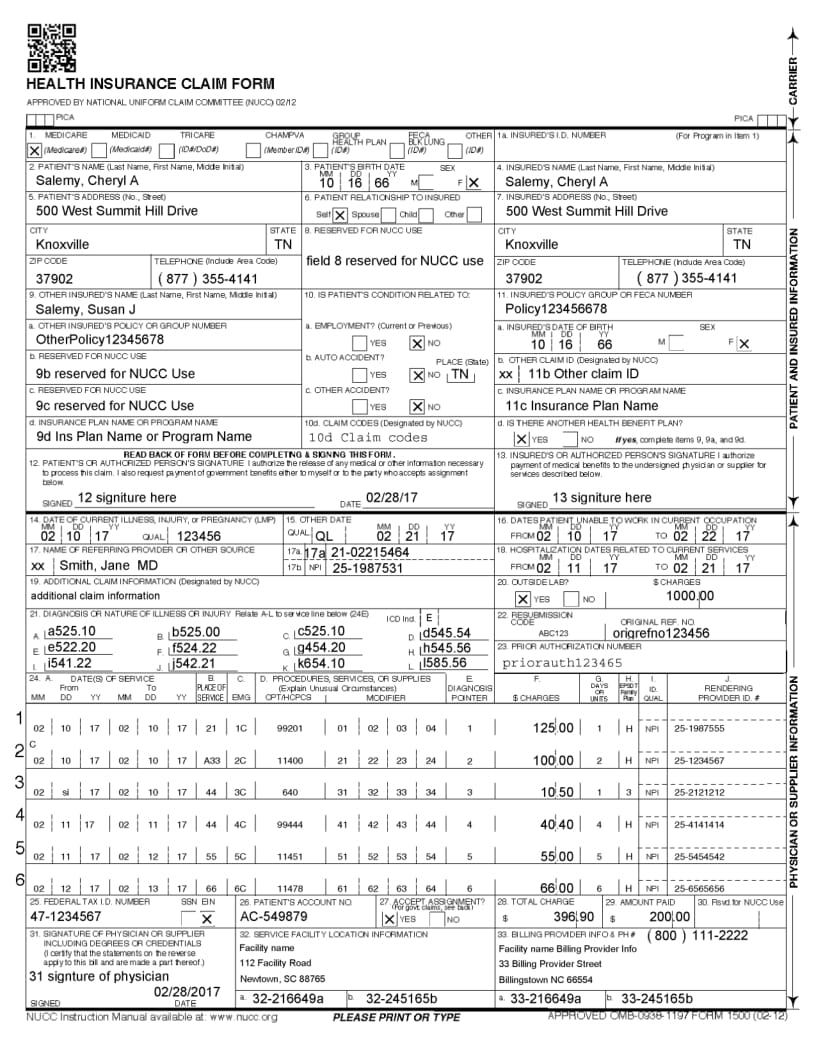
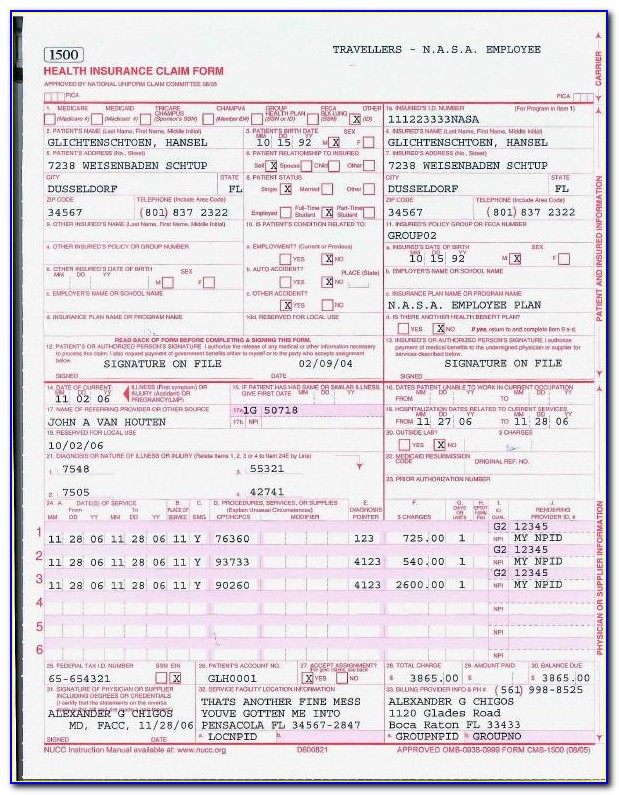
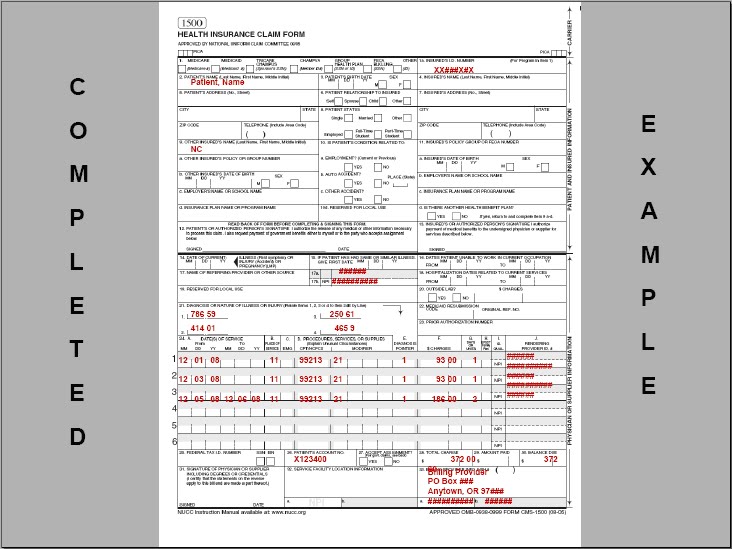
Completed Cms-1500 Form Sample 2020 - The form is used by physicians and allied health professionals to submit claims for medical services. Sign up to get the latest information about your choice of cms topics. You'll see instructions on how to complete the field. Insured’s address (no., street) city state zip code telephone (include area code) 11. Web cms 1500 dynamic list information. Easily fill out pdf blank, edit, and sign them. Refer to the physical therapy section of this manual for detailed policy information. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose. The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Web we are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs.
Last updated wed, 04 jan 2023 13:36:02 +0000. These instructions represent the minimum requirements for using this form to. All items must be completed unless otherwise noted in these instructions. For additional claim preparation information, refer to the forms: Web we are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. Insured’s address (no., street) city state zip code telephone (include area code) 11. Web cms 1500 dynamic list information. It can be purchased in any version required by calling the u.s. Sign up to get the latest information about your choice of cms topics. Web the 1500 health insurance claim form (1500 claim form) is in the public domain.
It is also used for submitting claims to many. Refer to the physical therapy section of this manual for detailed policy information. Choose the correct version of the editable pdf form from the list and get started filling it out. By most private insurance companies. Insured’s policy group or feca number a. The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Save or instantly send your ready documents. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. You can decide how often to. Insured’s address (no., street) city state zip code telephone (include area code) 11.

Cms 1500 Form 0212 Software Universal Network
You'll see instructions on how to complete the field. Web physician office sample cms 1500 claim form | entyvio® (vedolizumab) subject: The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Insured’s policy group or feca number a. You may also click in any field for more detailed instructions.

SAMPLE CMS 1500 form CMS 1500 claim form and UB 04 form
The form is used by physicians and allied health professionals to submit claims for medical services. Insured’s name (last name, first name, middle initial) 7. Web find and fill out the correct sample cms 1500 form completed. You may also click in any field for more detailed instructions. This document is intended to be a guide for completing the 1500.

Nucc Org Images Stories Pdf 1500 Claim Form Instruction Manual 2012
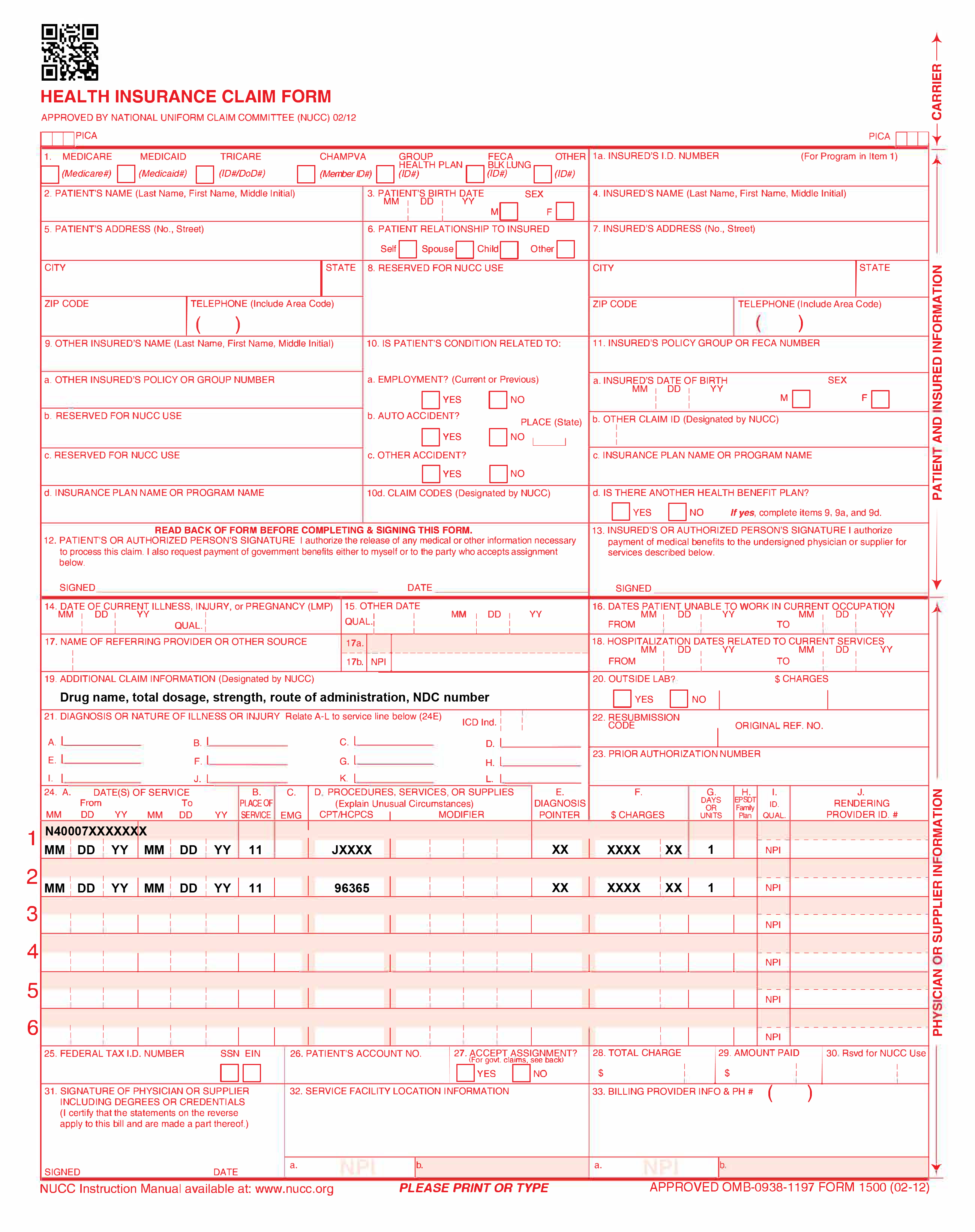
Physician office sample cms 1500 claim form. Enter the acquisition cost for pharmaceutical or radiopharmaceutical diagnostic imaging agents or for therapeutic radionuclides. You'll see instructions on how to complete the field. All items must be completed unless otherwise noted in these instructions. Insured’s address (no., street) city state zip code telephone (include area code) 11.
Processing CMS 1500 forms
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. See important safety information and prescribing information. Web find and fill out the correct sample cms 1500 form completed. Insured’s policy.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. All items must be completed unless otherwise noted in these instructions. This document is intended to be a guide for completing.
Medicare.gov Form 5510 Form Resume Examples R35xpgE51n
The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Web cms 1500 dynamic list information. The form is used by physicians and allied health professionals to submit claims for medical services. These instructions represent the minimum requirements for using this form to. All items must be completed unless otherwise noted in.
Specialty Drug Resource Sample CMS Forms
The copy below relates tothe graphic at left and is intended as general guidance for completing the form. Web cms 1500 dynamic list information. Easily fill out pdf blank, edit, and sign them. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Insured’s name (last name, first name, middle initial) 7. Insured’s address (no., street) city state zip code telephone (include area code) 11. The form is used by physicians and allied health professionals to submit claims for medical services. Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents.
Completed CMS 1500 form CMS 1500 claim form and UB 04 form
Web the 1500 health insurance claim form (1500 claim form) is in the public domain. Choose the correct version of the editable pdf form from the list and get started filling it out. Authority to collect information is in section 205(a), 1862, 1872 and 1874 of the social security act as amended, 42 cfr 411.24(a) and 424.5(a) (6), and The.

Sample Cms 1500 Form Filled Out Form Resume Examples 05KA75m8wP
Choose the correct version of the editable pdf form from the list and get started filling it out. The nucc has developed this general instructions document for completing the 1500claim form. By most private insurance companies. These instructions represent the minimum requirements for using this form to. Number (for program in item 1) 4.
You May Also Click In Any Field For More Detailed Instructions.
Sign up to get the latest information about your choice of cms topics. It can be purchased in any version required by calling the u.s. Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them.
This Document Is Intended To Be A Guide For Completing The 1500 Claim Form And Not Definitive Instructions For This Purpose.
All items must be completed unless otherwise noted in these instructions. Web we are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. Web cms 1500 dynamic list information. You can decide how often to.
Insured’s Policy Group Or Feca Number A.
Authority to collect information is in section 205(a), 1862, 1872 and 1874 of the social security act as amended, 42 cfr 411.24(a) and 424.5(a) (6), and It is also used for submitting claims to many. Choose the correct version of the editable pdf form from the list and get started filling it out. Insured’s name (last name, first name, middle initial) 7.
Number (For Program In Item 1) 4.
By most private insurance companies. Insured’s address (no., street) city state zip code telephone (include area code) 11. For additional claim preparation information, refer to the forms: Physician office sample cms 1500 claim form.