Driver Clearance Form
Driver Clearance Form - Web requirements to be cleared drivers must: Web able to procure a letter of clearance from their previous operator for whatever reason. Printed name of certified medical examiner: Web this driver medical evaluation form. For drivers with an oregon driving record (driver's license) in the three (3) preceding years, the service center will request records from the oregon dmv. Submit the driver's clearance form. Date of birth:(print) date clearance needed: _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator. There will be a $5.00 charge to the department. Web as defined in § 382.107, who is familiar with the driver’s medical history and has advised the driver that the substance will not adversely affect the driver’s ability to safely operate a cmv.
Club & activity employment type (fte, cont, vol, stud): Date of birth:(print) date clearance needed: Web this driver medical evaluation form. For drivers with an oregon driving record (driver's license) in the three (3) preceding years, the service center will request records from the oregon dmv. Printed name of certified medical examiner: Signature of certified medical examiner: There will be a $5.00 charge to the department. _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator. Web able to procure a letter of clearance from their previous operator for whatever reason. Web driver clearance this letter is to confirm that my driver mr./mrs.
Web the driver submits to a diabetic examination every 6 months, and submits the results of the examination and the results of the hemoglobin a1c (hba1c) test on a form provided by the department.the health care provider reviewing the diabetic examination shall be familiar with the person’s past diabetic history for 24 months or have access to. Web drivers license number:(print) state of issue: Submit the driver's clearance form. Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. I hereby waive grab from all liability that may result from the actions and behavior of the driver that may lead to undesirable transactions or circumstance. Web this driver medical evaluation form. _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator. Printed name of certified medical examiner: Web requirements to be cleared drivers must: Date of birth:(print) date clearance needed:
FREE 12+ Company Exit Clearance Forms in PDF
Web requirements to be cleared drivers must: Club & activity employment type (fte, cont, vol, stud): Date of birth:(print) date clearance needed: Web this driver medical evaluation form. Submit the driver's clearance form.

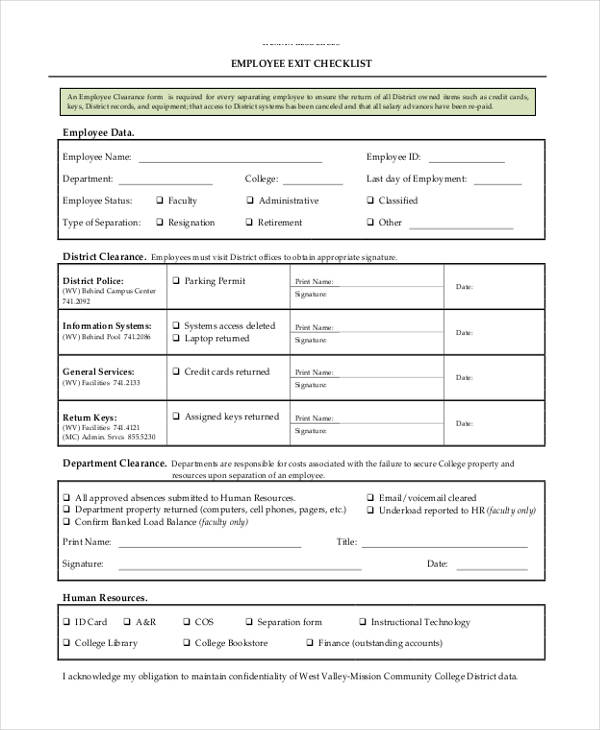
FREE 10+ Employee Clearance Forms in PDF MS Word
Web this driver medical evaluation form. There will be a $5.00 charge to the department. Signature of certified medical examiner: Submit the driver's clearance form. Web able to procure a letter of clearance from their previous operator for whatever reason.

Medical Clearance Form copy Kitsilano Neighbourhood House
Date of birth:(print) date clearance needed: Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. Web drivers license number:(print) state of issue: _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator..
FREE 17+ Employee Clearance Forms in PDF MS Word Excel
Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator. Web this driver medical evaluation form. Web as defined in § 382.107, who.
FREE 10+ Sample Employee Clearance Forms in PDF MS Word Excel
Web this driver medical evaluation form. Date of birth:(print) date clearance needed: Signature of certified medical examiner: This letter is to confirm that my driver mr./ms_____has no pending financial obligation current management (peer/operator), hence is free to transfer to another peer/operator. There will be a $5.00 charge to the department.
FREE 21+ Employee Clearance Forms in PDF Excel MS Word
Web the driver submits to a diabetic examination every 6 months, and submits the results of the examination and the results of the hemoglobin a1c (hba1c) test on a form provided by the department.the health care provider reviewing the diabetic examination shall be familiar with the person’s past diabetic history for 24 months or have access to. Club & activity.
FREE 14+ Application Clearance Forms in PDF Word
Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. Web this driver medical evaluation form. Web as defined in § 382.107, who is familiar with the driver’s medical history and has advised the driver that the substance will not.

District Driver Clearance Form Arena Elementary School
Submit the driver's clearance form. _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator. Web the driver submits to a diabetic examination every 6 months, and submits the results of the examination and the results of the hemoglobin a1c (hba1c) test on a form provided by the department.the health care provider reviewing.
FREE 11+ Employee Clearance Forms in MS Word
There will be a $5.00 charge to the department. For drivers with an oregon driving record (driver's license) in the three (3) preceding years, the service center will request records from the oregon dmv. This letter is to confirm that my driver mr./ms_____has no pending financial obligation current management (peer/operator), hence is free to transfer to another peer/operator. Date of.

District Driver Clearance Form Arena Elementary School
Date of birth:(print) date clearance needed: Web as defined in § 382.107, who is familiar with the driver’s medical history and has advised the driver that the substance will not adversely affect the driver’s ability to safely operate a cmv. Club & activity employment type (fte, cont, vol, stud): This letter is to confirm that my driver mr./ms_____has no pending.
This Letter Is To Confirm That My Driver Mr./Ms_____Has No Pending Financial Obligation Current Management (Peer/Operator), Hence Is Free To Transfer To Another Peer/Operator.
Web driver clearance this letter is to confirm that my driver mr./mrs. Web as defined in § 382.107, who is familiar with the driver’s medical history and has advised the driver that the substance will not adversely affect the driver’s ability to safely operate a cmv. Signature of certified medical examiner: Web drivers license number:(print) state of issue:
Printed Name Of Certified Medical Examiner:
Web able to procure a letter of clearance from their previous operator for whatever reason. Club & activity employment type (fte, cont, vol, stud): There will be a $5.00 charge to the department. _____ has no pending financial obligation current management (peer/operator), hence, is free to transfer to another peer/operator.
I Hereby Waive Grab From All Liability That May Result From The Actions And Behavior Of The Driver That May Lead To Undesirable Transactions Or Circumstance.
Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. Web this driver medical evaluation form. Submit the driver's clearance form. Web the driver submits to a diabetic examination every 6 months, and submits the results of the examination and the results of the hemoglobin a1c (hba1c) test on a form provided by the department.the health care provider reviewing the diabetic examination shall be familiar with the person’s past diabetic history for 24 months or have access to.
For Drivers With An Oregon Driving Record (Driver's License) In The Three (3) Preceding Years, The Service Center Will Request Records From The Oregon Dmv.
Web requirements to be cleared drivers must: Date of birth:(print) date clearance needed: