Florida Medicaid Prior Authorization Form
Florida Medicaid Prior Authorization Form - Prescriber license # (me, os, arnp, pa) Electronic prior authorizations [ 20.7 kb ] drug criteria Brand name drug preferred list [ 79.4 kb ] updated july 21, 2023. Web updated june 02, 2022. Mail or fax information to: An incomplete form may be returned. Faqs [ 131.1 kb ] provider enrollment. Form must be completed in full. Early and periodic screening, diagnostic and treatment (epsdt) benefit. All relevant sections of the antidepressant prior authorization form must be complete.
Prescriber license # (me, os, arnp, pa) Form must be completed in full. Early and periodic screening, diagnostic and treatment (epsdt) benefit. Brand name drug preferred list [ 79.4 kb ] updated july 21, 2023. Web pharmacy prior authorization forms. Mail or fax information to: An incomplete form may be returned. Recipient’s medicaid id# date of birth (mm/dd/yyyy) / / recipient’s full name. Faqs [ 131.1 kb ] provider enrollment. An incomplete form may be returned.
Faqs [ 131.1 kb ] provider enrollment. Mail or fax information to: An incomplete form may be returned. Web updated june 02, 2022. For more information, an electronic prior authorization information sheet [ 20.7 kb ] is available on medicaid’s website. Certain injectable and specialty medications require prior authorization. Early and periodic screening, diagnostic and treatment (epsdt) benefit. Send request to our utilization management department. The evaluation and progress notes must document target symptoms and behaviors. Form must be completed in full.
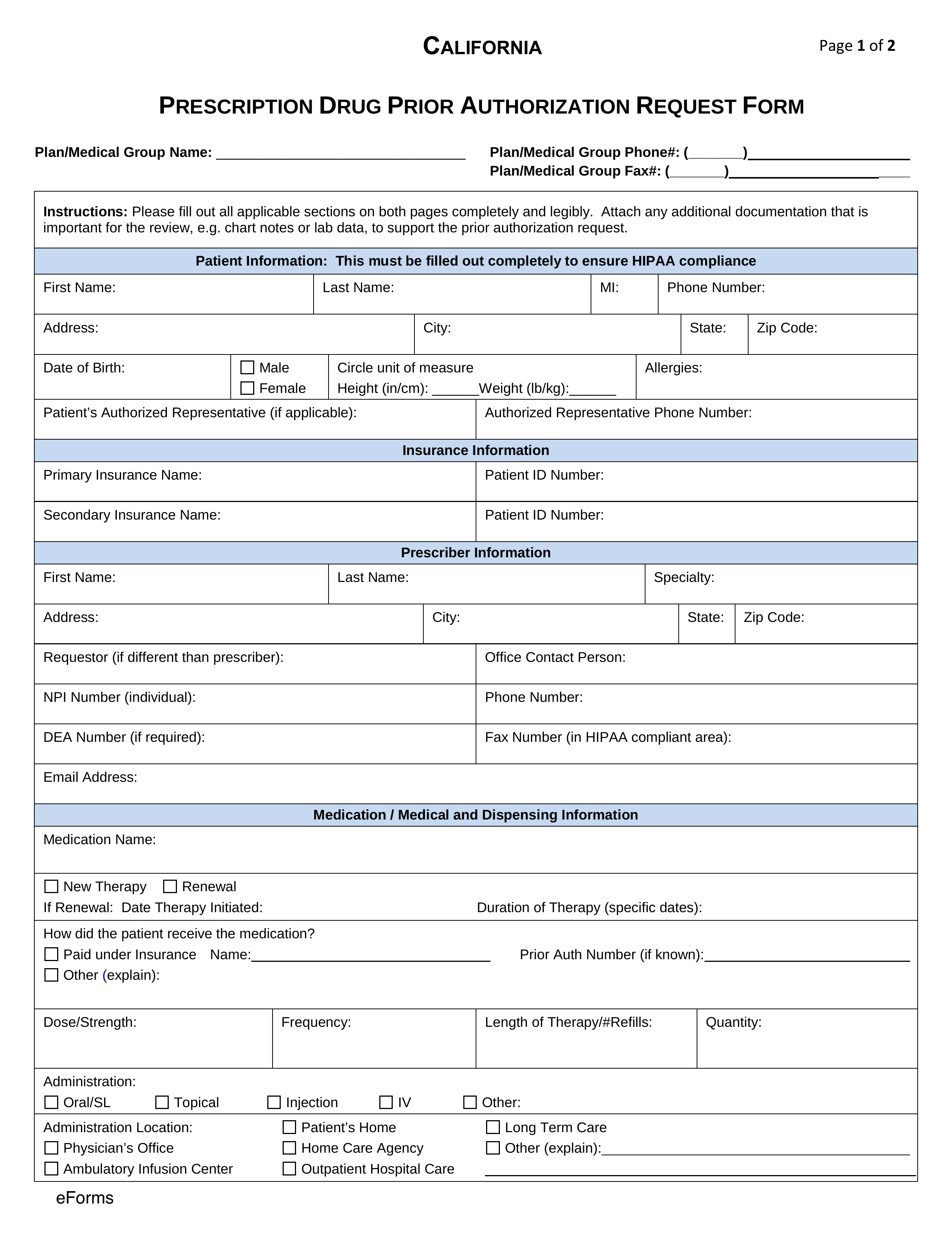
Free California Medicaid Prior (Rx) Authorization Form PDF eForms
Electronic prior authorizations [ 20.7 kb ] drug criteria Form must be completed in full. An incomplete form may be returned. Certain injectable and specialty medications require prior authorization. Medicare elective inpatient prior authorization form (pdf) medicare outpatient prior authorization form (pdf).
Florida Medicaid Tax Forms Form Resume Examples X42M4bMAVk
Mail or fax information to: Form must be completed in full. Brand name drug preferred list [ 79.4 kb ] updated july 21, 2023. Early and periodic screening, diagnostic and treatment (epsdt) benefit. Web medicaid home health (hh) services.
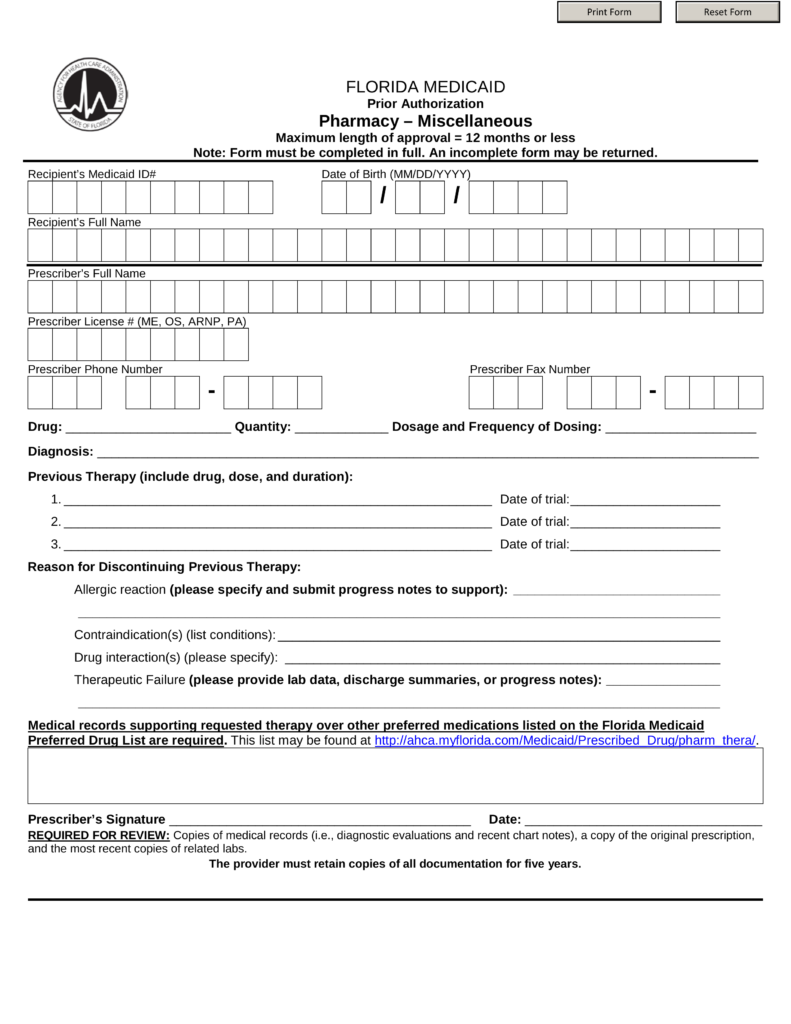
Free Florida Medicaid Prior (Rx) Authorization Form PDF eForms
Web updated june 02, 2022. Recipient’s medicaid id# date of birth (mm/dd/yyyy) / / recipient’s full name. Certain injectable and specialty medications require prior authorization. The evaluation and progress notes must document target symptoms and behaviors. Form must be completed in full.
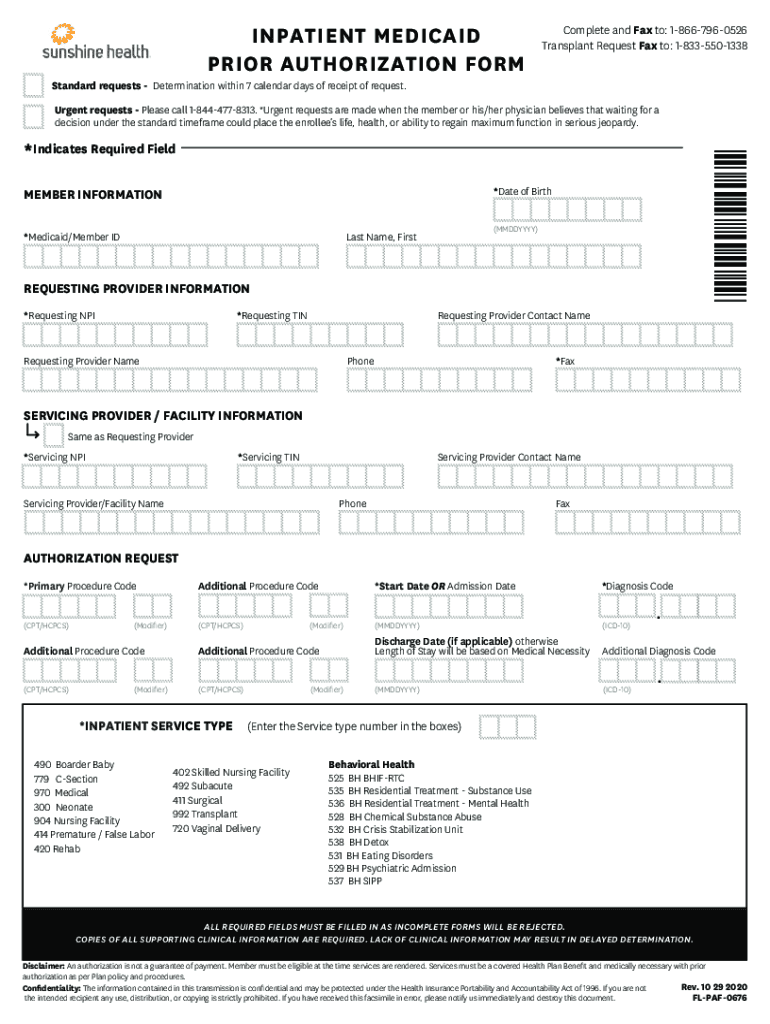
Priority Health Inpatient Authorization Form Fill Out and Sign
Faqs [ 131.1 kb ] provider enrollment. Web updated june 02, 2022. Mail or fax information to: Items on this list will only be dispensed after prior authorization from molina healthcare. Form must be completed in full.
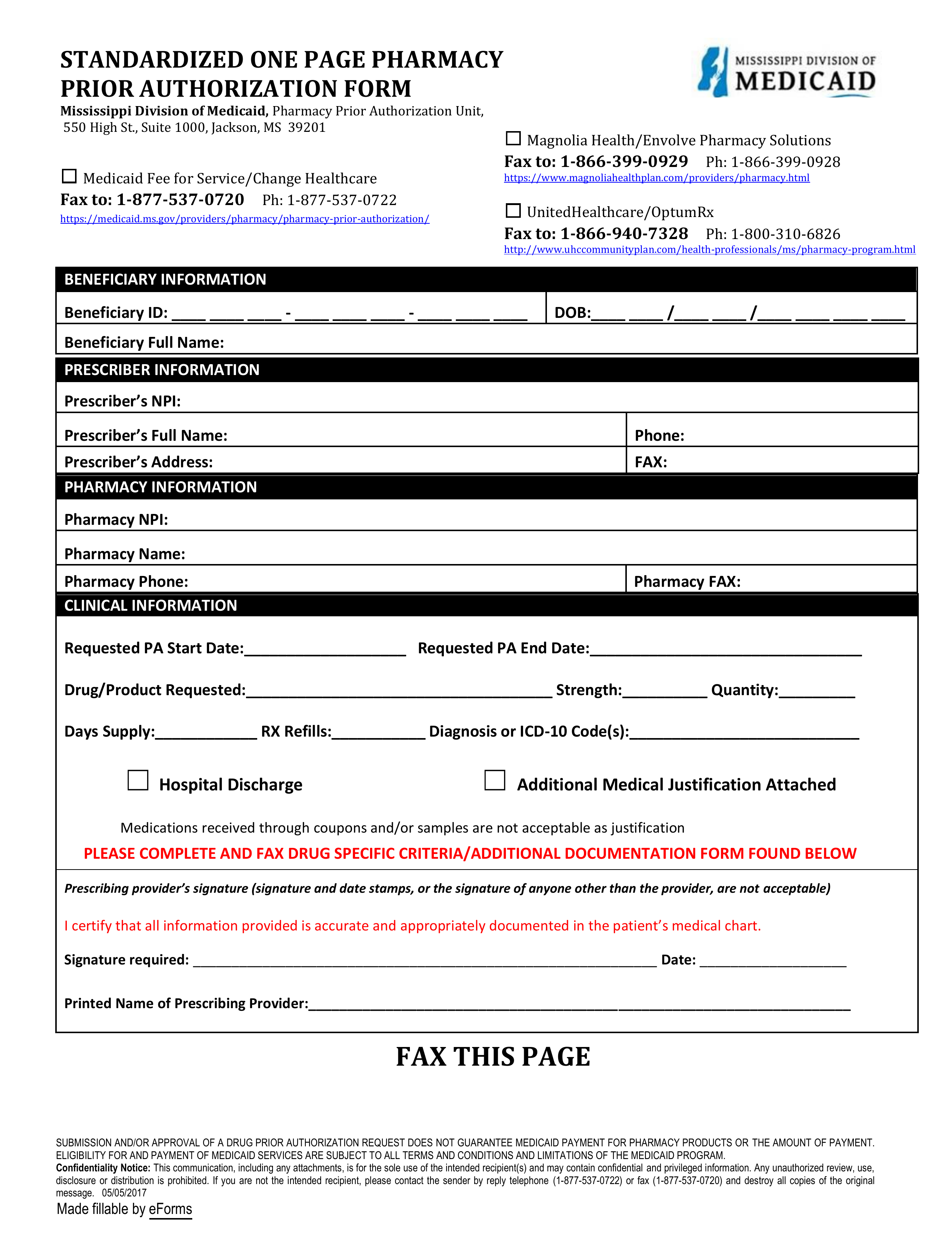
Free Mississippi Medicaid Prior (Rx) Authorization Form PDF eForms
Web the most current antidepressant prior authorization request form is required for review. Items on this list will only be dispensed after prior authorization from molina healthcare. An incomplete form may be returned. Web pharmacy prior authorization forms. Medicare elective inpatient prior authorization form (pdf) medicare outpatient prior authorization form (pdf).

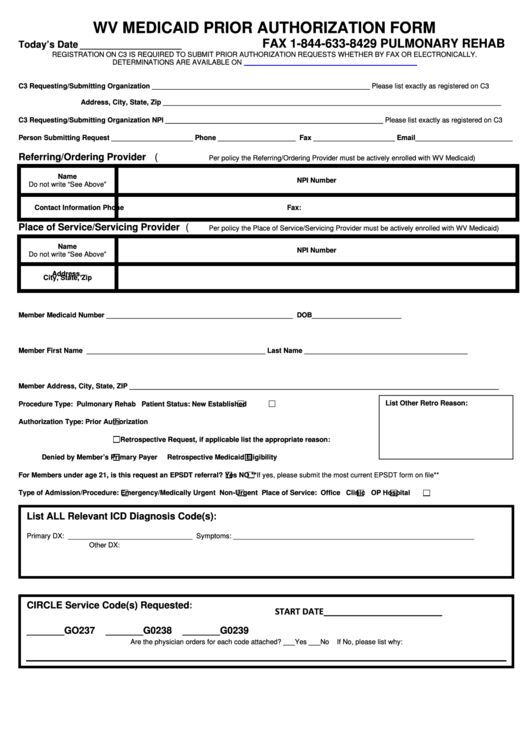
West Virginia Medicaid Prior Authorization Form Form Resume
Medicaid outpatient prior authorization form (pdf) durable medical equipment home health and home infusion referral form (pdf) medicare. The evaluation and progress notes must document target symptoms and behaviors. An incomplete form may be returned. Recipient’s medicaid id# date of birth (mm/dd/yyyy) / / recipient’s full name. Prescriber license # (me, os, arnp, pa)
Top 26 Medicaid Prior Authorization Form Templates free to download in
Medicare elective inpatient prior authorization form (pdf) medicare outpatient prior authorization form (pdf). The evaluation and progress notes must document target symptoms and behaviors. Items on this list will only be dispensed after prior authorization from molina healthcare. Mail or fax information to: Medicaid outpatient prior authorization form (pdf) durable medical equipment home health and home infusion referral form (pdf).
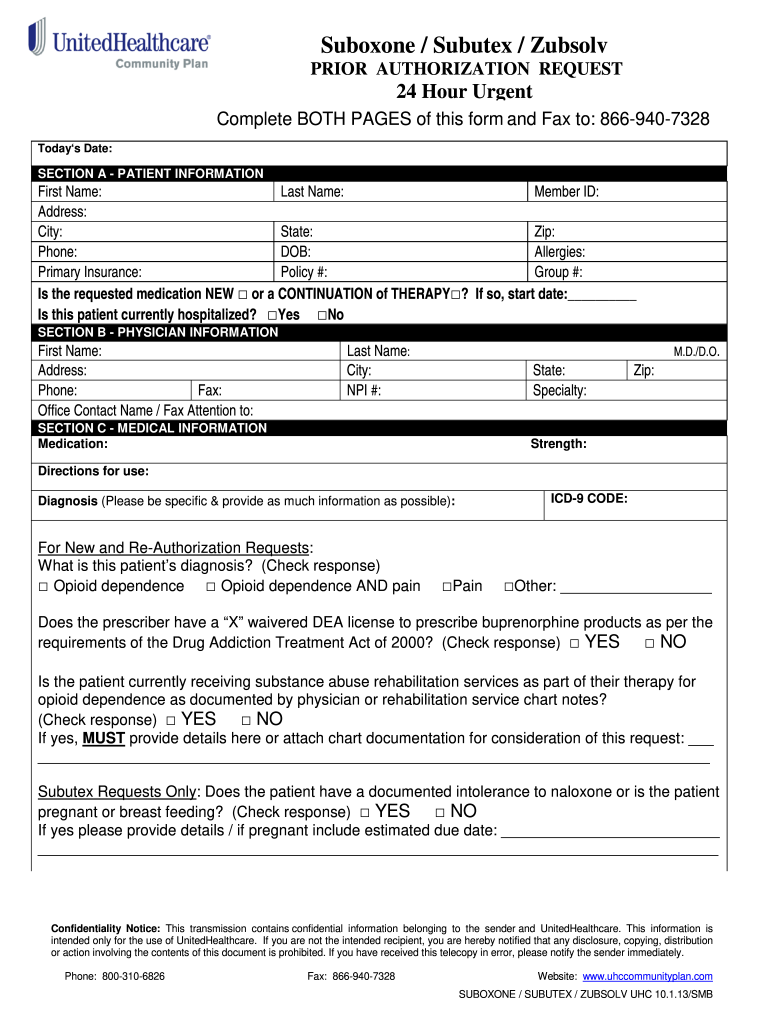
Prior Authorization Request Form Fill Online, Printable, Fillable
Items on this list will only be dispensed after prior authorization from molina healthcare. All relevant sections of the antidepressant prior authorization form must be complete. The evaluation and progress notes must document target symptoms and behaviors. Brand name drug preferred list [ 79.4 kb ] updated july 21, 2023. Web medicaid home health (hh) services.
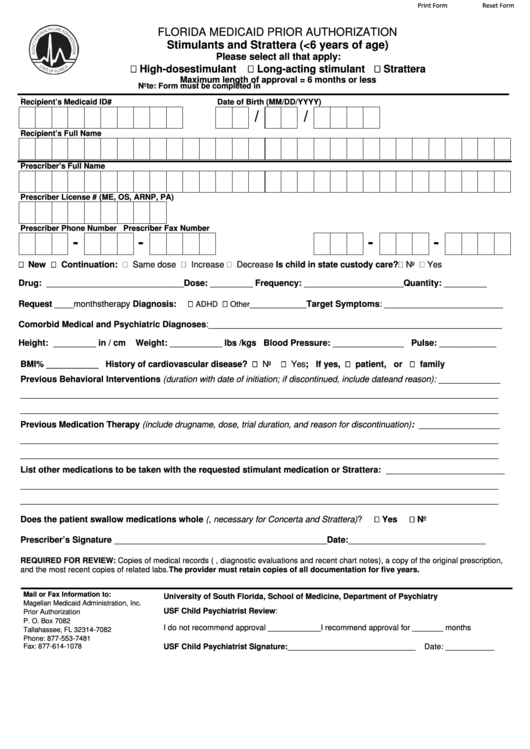
Fillable Florida Medicaid Prior Authorization printable pdf download
All relevant sections of the antidepressant prior authorization form must be complete. Form must be completed in full. Medicare elective inpatient prior authorization form (pdf) medicare outpatient prior authorization form (pdf). Recipient’s medicaid id# date of birth (mm/dd/yyyy) / / recipient’s full name. Form must be completed in full.

Prior authorization form for caremark
Mail or fax information to: Web updated june 02, 2022. Certain injectable and specialty medications require prior authorization. Web medicaid home health (hh) services. Brand name drug preferred list [ 79.4 kb ] updated july 21, 2023.
Early And Periodic Screening, Diagnostic And Treatment (Epsdt) Benefit.
Recipient’s medicaid id# date of birth (mm/dd/yyyy) / / recipient’s full name. An incomplete form may be returned. An incomplete form may be returned. Medicare elective inpatient prior authorization form (pdf) medicare outpatient prior authorization form (pdf).
Faqs [ 131.1 Kb ] Provider Enrollment.
Mail or fax information to: Items on this list will only be dispensed after prior authorization from molina healthcare. Send request to our utilization management department. Web the most current antidepressant prior authorization request form is required for review.
The Evaluation And Progress Notes Must Document Target Symptoms And Behaviors.
Web pharmacy prior authorization forms. Form must be completed in full. Certain injectable and specialty medications require prior authorization. For more information, an electronic prior authorization information sheet [ 20.7 kb ] is available on medicaid’s website.
Brand Name Drug Preferred List [ 79.4 Kb ] Updated July 21, 2023.
Prescriber license # (me, os, arnp, pa) Web florida medicaid preferred drug program. Electronic prior authorizations [ 20.7 kb ] drug criteria Medicaid outpatient prior authorization form (pdf) durable medical equipment home health and home infusion referral form (pdf) medicare.